
CME INDIA Presentation by Dr. A. N. Rai, MD, MRCP (U.K), FRCP (Glasgow)FICP, FICC, FICN, Former Prof. & Head Department of Medicine and Principal, ANMCH, Gaya, Chairman of AIMS, Gayajee, Bihar.
Based on a presentation at ISLET-2026, Bengaluru on March 22.
Case 1:
- Elderly Diabetic Male presenting with severe burning pain in chest with sweating and restlessness for 3 hours came to AIMS emergency for admission and treatment.
- Before he could be shifted to ICU, he had sudden fit with convulsions lasting for few second. His pulse was feeble and BP not recordable.
- Blood Profile CBC- With in normal limits Blood Sugar- 226 (R)
Serum Creatinine – 2.80
Serum K – 6.2 Serum Sodium – 131.5 - ECHO
- Normal chamber dimension. Basal mid Inf wall hypokinetic,
- 2DLV EF = 40%. TAPSE = 16 mm. No MR/AR/TR. IVC = 23 mm & >50% collapsible.
- Final impression
- CAD, RWMA IN RCA territory, moderate LV systolic dysfunction,
- LVEF = 40%.
Diagnosis?
- Management
- Patient was put on TPI and Hyperkalemia was managed medically by giving IV Calcium
- Nebulization and IV glucose and Insulin.
- In addition to dual Antiplatelet and 80mg Atorvastatin he was Thrombolysis by Retiplase.
- His diabetes was managed by insulin
- He recovered within 24 hours.
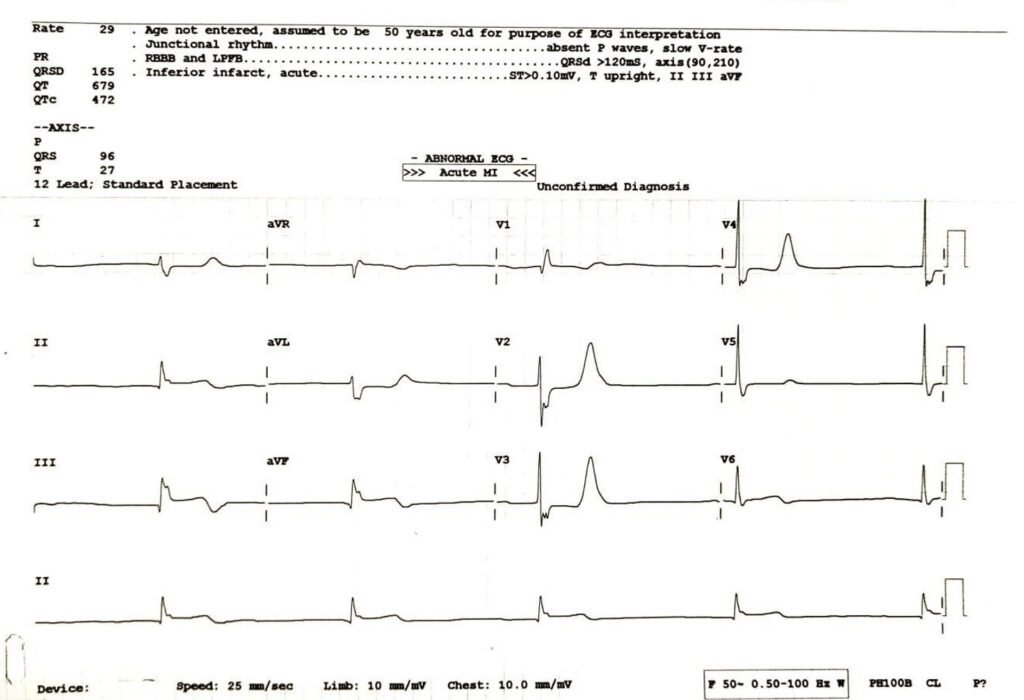
- His ECG is given below:
Electrolytes
- Serum Sodium: 137.80 mmol/L (135.00 – 155.00 mmol/L)
- Serum Potassium: 4.09 mmol/L (3.50 – 5.00 mmol/L)
- Serum Chloride: 101.10 mmol/L (96.00 – 106.00 mmol/L)
Renal Parameters
- Blood Urea: 82.00 mg/dL (10.00 – 40.00 mg/dL)
- Serum Creatinine: 1.95 mg/dL (0.70 – 1.30 mg/dL)
Glycaemic Status
- Blood Sugar (Fasting): 174.00 mg/dL (70.00 – 110.00 mg/dL)
Diagnosis
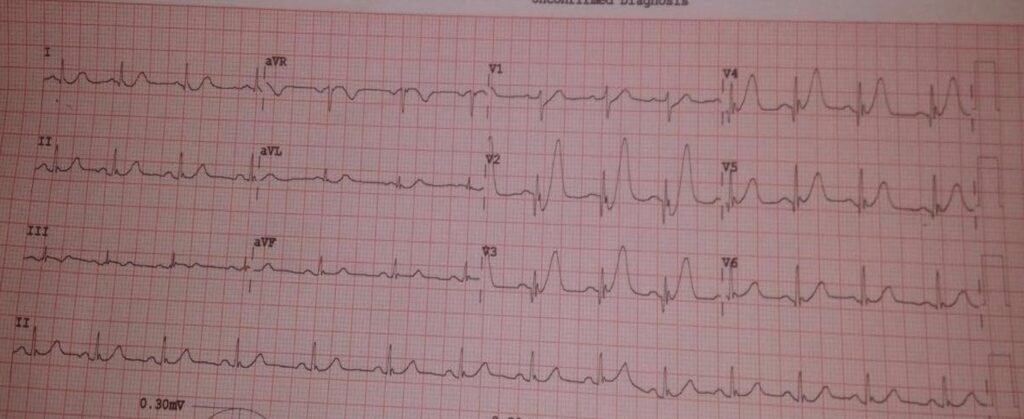
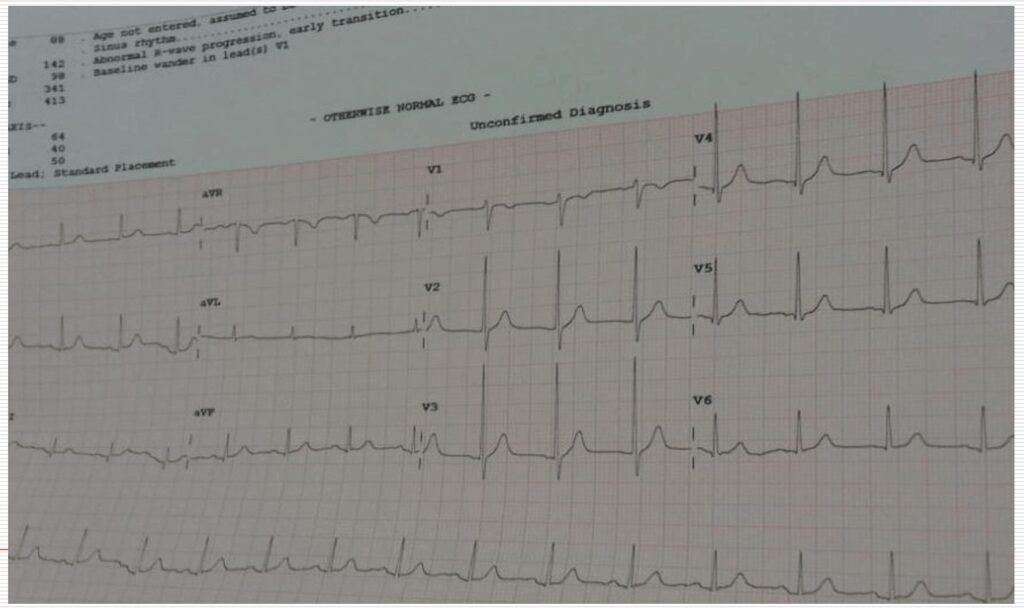
Case no 1 is Classical Inferior STEMI with following ECG features of Hyperkalaemia .
- Tall T wave in Precordial Leads
- Absent P wave
- Bradycardia
- BRASH Syndrome features are:
- Bradycardia
- Renal failure
- AV Blocking drug
- Shock
- Hyperkalaemia
Since this patient was not on AV Blocking Drugs like Beta Blocker or Calcium Channel Blocker at the time of admission when the ECG was recoded, diagnosis of BRASH Syndrome is unlikely.
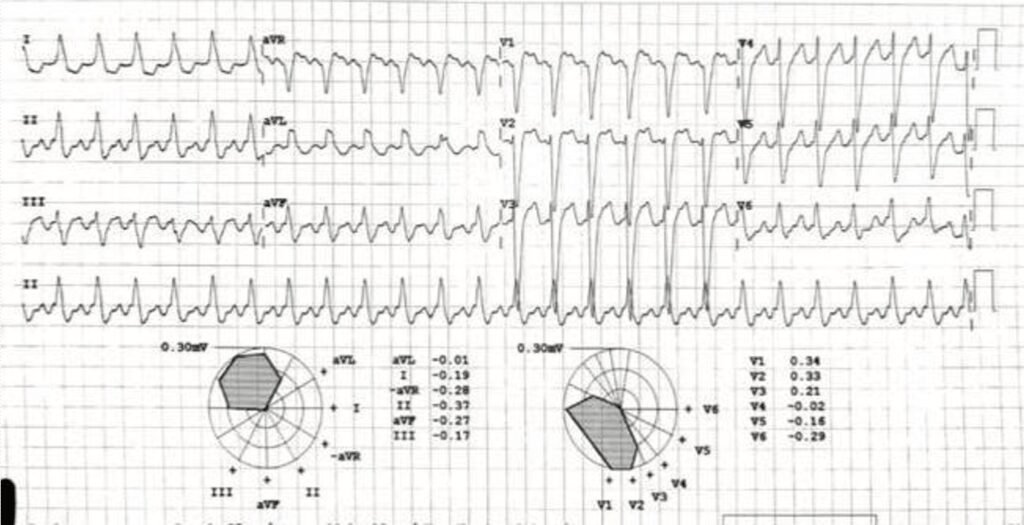
Case 2:
ECG of middle-aged Diabetic Male presenting as severe chest pain for 3 hours.
- Diagnosis and Management.
Diagnosis
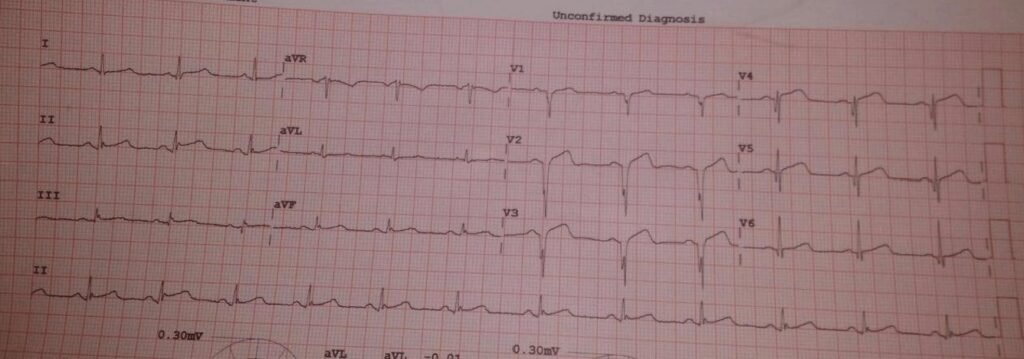
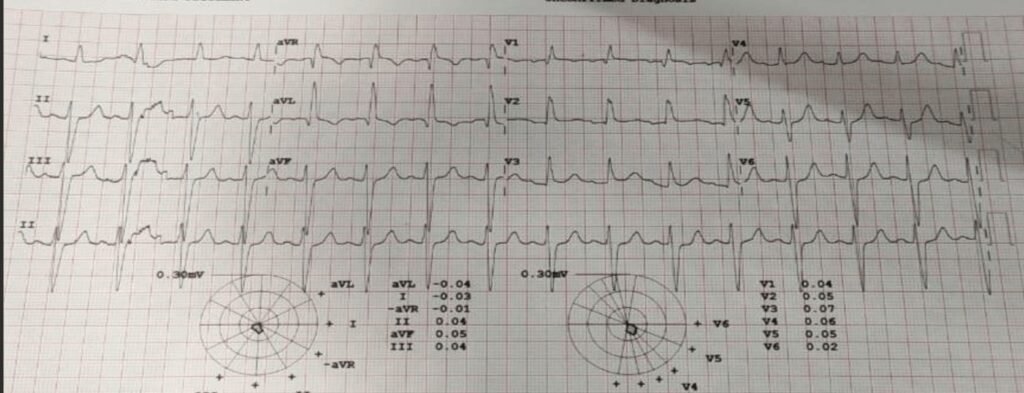
- The de Winter ECG pattern is an anterior STEMI equivalent that presents without obvious ST segment elevation. First reported by de winter in 2008.
- Key diagnostic features of de Winter pattern include ST depression and peaked T waves in the precordial leads.
- de Winter pattern is seen in 2% of acute LAD occlusions.
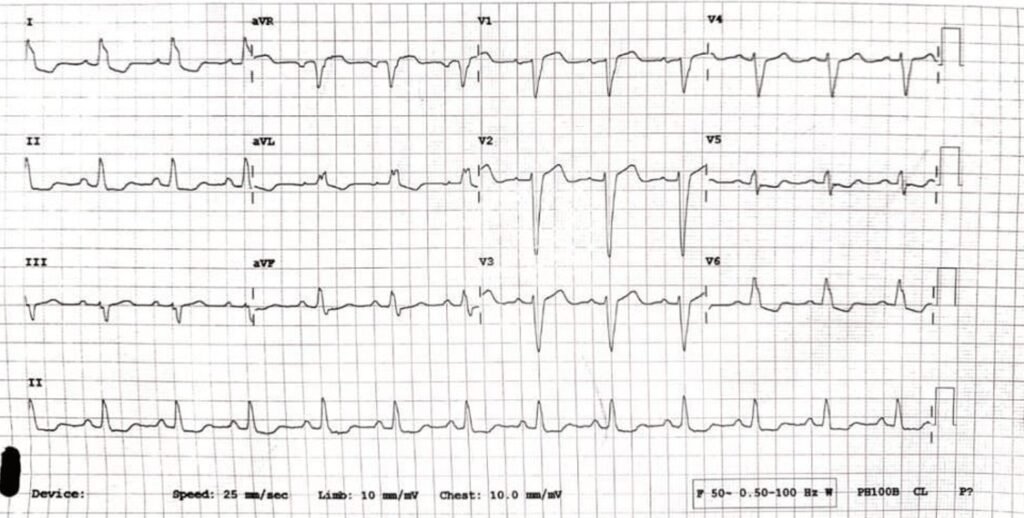
Management:
- Thrombolysis
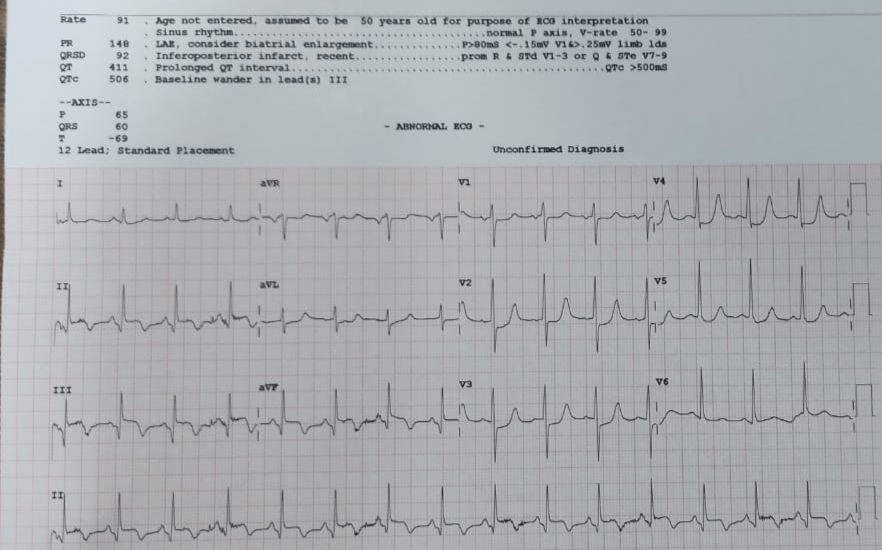
- Post Thrombolysis ECG:
Case 3:
- 35 years old Diabetic male was admitted with H/O weakness and giddiness since morning.
- O/E Pulse 40/min, BP 160/100
- His ECG given below:
- Investigations
- Blood Sugar 300mg/dl
- Serum Creatinine 3.5mg/dl
- Serum Potassium 6.5 millieq/L
- Patient was managed conservatively by giving IV calcium and insulin.
- He was advising Dialysis when he did not show improvement but refused. His ECG 6 hours latter given below:
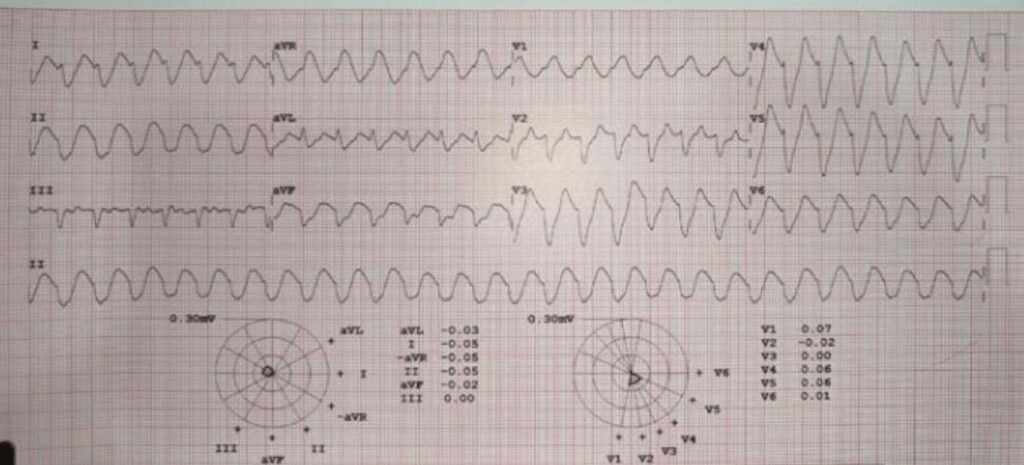
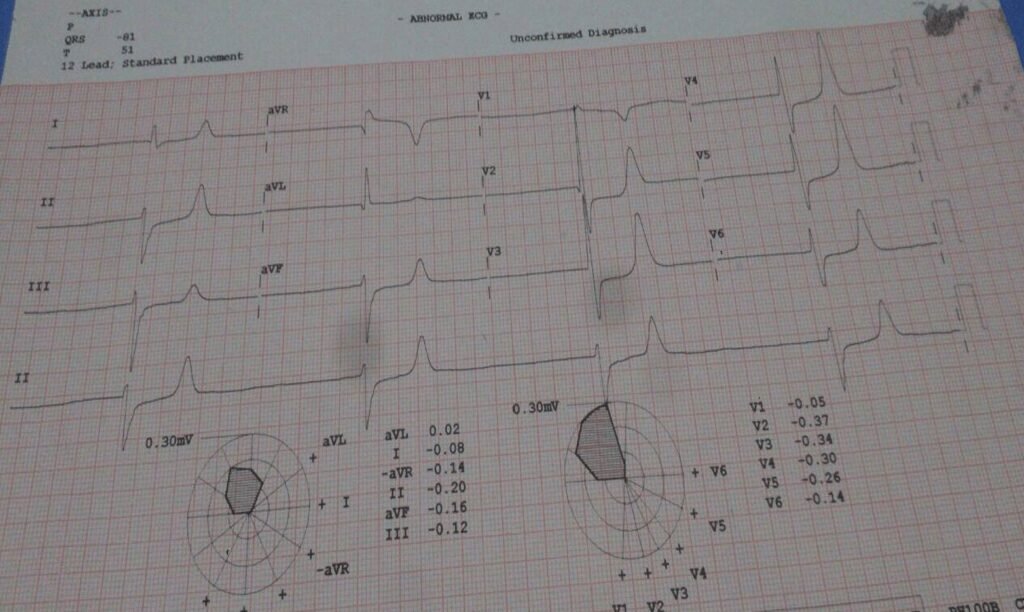
Diagnosis:
- This is Sine wave due to merger of wide QRS with wide T wave.
serum potassium 7.7 millieq/L. - Patient was saved after he agreed for dialysis.
Post recovery ECG with potassium 5millieq/L:
Case 3:
- Elderly Diabetic male presenting with fits for 1 Day. Diagnosis? Management
- ECG Given below:
- Diagnosis: Standard Masquerading BBB Standard MBBB
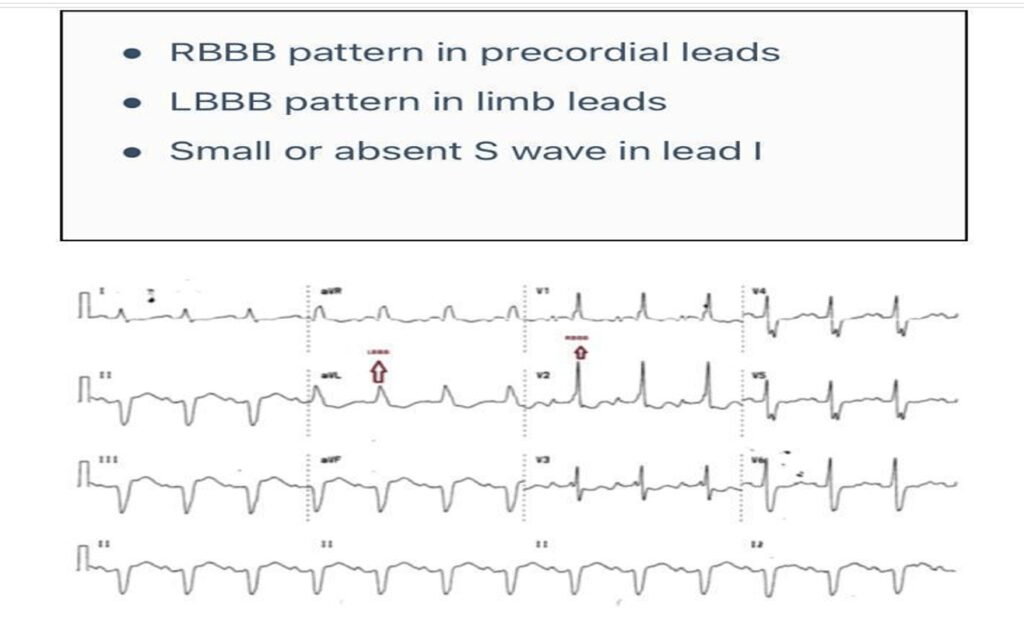
Precordial MBBB
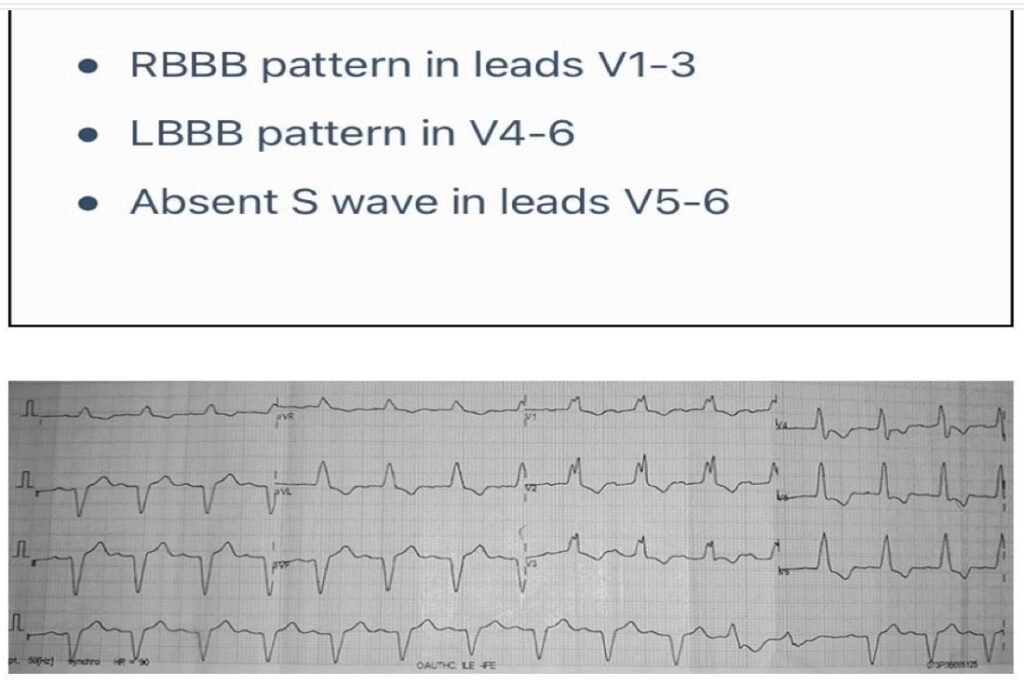
Management: Patient requires urgent cardiac pacing since Masquerading BBB suggest high degree Bifascicular Block.
Case 5:
- Middle aged Diabetic lady presenting as sudden chest pain, palpitation, giddiness with sweating and restlessness for 1.5 hours.
- O/E she had features of shock with cold limbs with absent pulse and BP.
- Her ECG is given below:
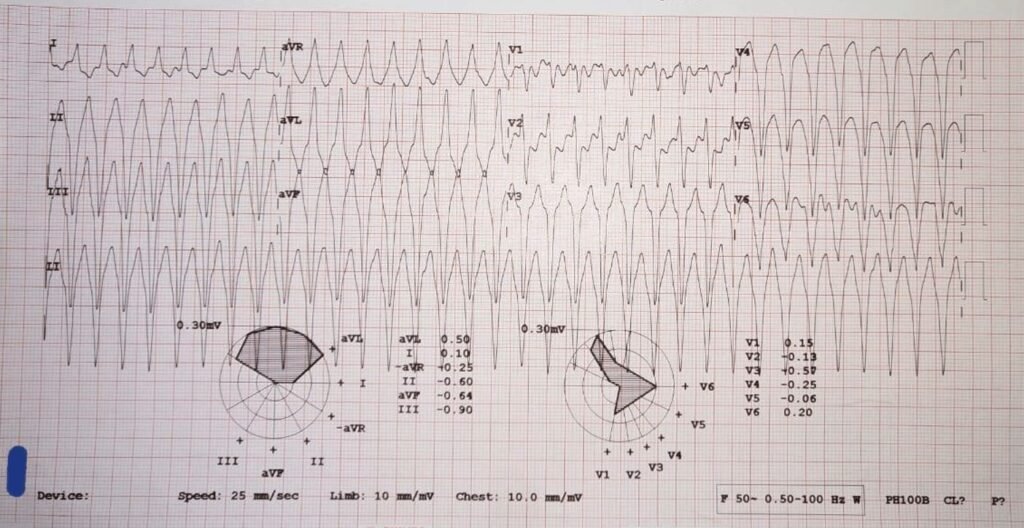
- What is Diagnosis?
- How will you Manage?
- Diagnosis: VT.
- Management: DC Shock.
- Post DC Shock ECG given below:
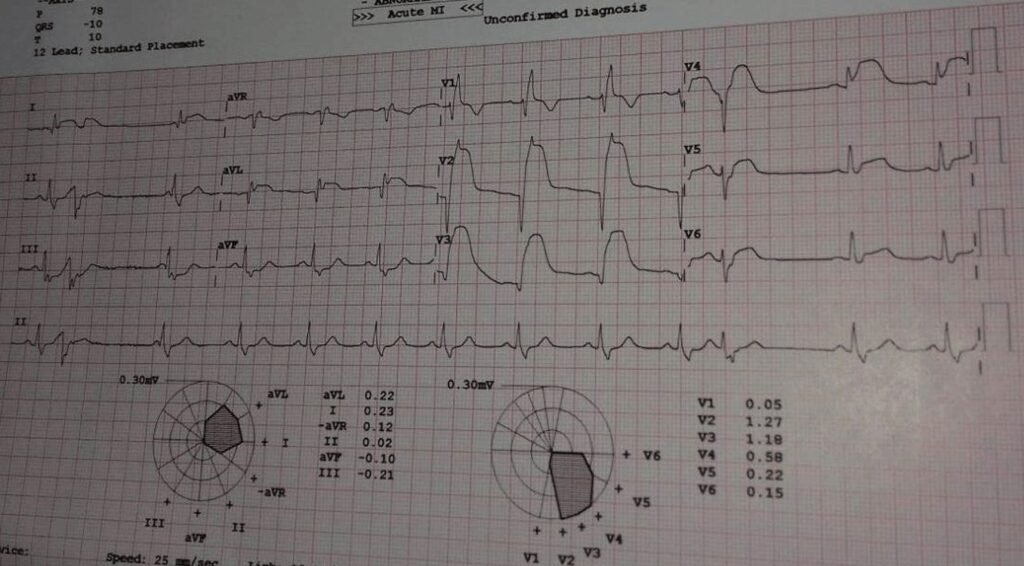
- Post DC Shock Diagnosis and Management
- Post DC Shock ECG shows Acute Anterior STEMI
- Management:
- Primary Angioplasty.
- Thrombolysis, if there is no facility for Angioplasty.
- Anti-Diabetic medication.
Case 6:
- Elderly Diabetic Female admitted in ICU of AIMS with sudden Palpitations with severe Breathlessness for 4 hours.
- She gave past h/o Breathlessness for 3 years.
- CBC: Hb 10.5 gm, TC, DC and Platelets within normal limits Blood Sugar: 140gm (F), HbA1c 7.5, Serum Creatinine 1.0 gm
- Her ECG and X-ray chest given below:

- Diagnosis
- DCMP with Global Hyperkinesia and LBBB with EF 30% DM, DCMP with Atrial Flutter and Heart Failure.
- Patient was given IV Lasix and, Verapamil 40mg 2 stat and 1 tds, Amiodarone 200 mg bd and Enalapril 2.5 mg od, Dapagliflozin 10 mg od and Metformin 500 mg od
Her ECG next morning given below:
CME INDIA Learning Edge
🔴 Case 1 Acute Inferior Wall STEMI (RCA territory) with concomitant severe Hyperkalaemia mimicking/augmenting ECG change
Always suspect dual pathology in diabetics with CKD presenting with ACS—ischemia and electrolyte imbalance often coexist.
- Hyperkalaemia can significantly alter ECG morphology, sometimes mimicking or obscuring STEMI patterns, especially with tall T waves and absent P waves.
- Inferior STEMI (RCA territory) frequently presents with bradycardia due to SA/AV nodal ischemia—do not mislabel it as primary conduction disease.
- Sudden convulsions in ACS are often arrhythmic syncope equivalents caused by transient cerebral hypoperfusion, not primary seizures.
- In hemodynamically unstable patients, immediate stabilization of hyperkalaemia (IV calcium, insulin–glucose) is life-saving and should precede or accompany reperfusion.
- Severe hyperkalaemia (K⁺ >6 mmol/L) increases risk of fatal arrhythmias and can precipitate shock even before infarction is treated.
- Absence of AV nodal blocking drug exposure effectively rules out BRASH syndrome despite overlapping features.
- Insulin infusion in ACS with hyperglycaemia provides dual benefit—glycaemic control and intracellular potassium shift.
- Echo evidence of RWMA (inferior wall hypokinesia) confirms ischemic territory when ECG interpretation is confounded.
- Rapid correction of potassium with simultaneous reperfusion therapy leads to dramatic clinical recovery, as seen within 24 hours in this case.
👉 Key Point: “In ACS, always read the ECG through the lens of electrolytes—potassium can deceive before it kills.
🔴 Case 2: de Winter Pattern (Anterior STEMI Equivalent)
Final Clinical Pearls:
- ST depression with tall peaked T waves in V1–V6 = de Winter pattern, a STEMI equivalent indicating proximal LAD occlusion.
- Absence of ST elevation does NOT exclude acute coronary occlusion—this is a critical ECG trap.
- Seen in ~2% of LAD occlusions but carries the same urgency as STEMI.
- Immediate reperfusion (PCI/thrombolysis) is mandatory, not “NSTEMI protocol.”
- Diabetics are more prone to atypical ECG patterns due to autonomic dysfunction and diffuse ischemia.
👉 Key Point: “Not all STEMIs elevate—some hide in de Winter disguise.”
🔴 Case 3: Hyperkalaemia → Sine Wave ECG
Final Clinical Pearls:
- Progression from peaked T → widened QRS → sine wave = pre-arrest hyperkalaemia.
- Serum K⁺ >6.5–7 mEq/L is a cardiac emergency irrespective of symptoms.
- In diabetics with CKD, ECG changes often precede clinical deterioration.
- Medical therapy (Ca²⁺, insulin) is temporizing—definitive therapy is dialysis.
- Delay in dialysis converts reversible ECG changes into fatal ventricular arrhythmias.
👉 Key Point: “Sine wave ECG is not a rhythm—it is a countdown to cardiac arrest.”
🔴 Case 4: Masquerading Bundle Branch Block (MBBB)
Final Clinical Pearls:
- RBBB in precordial leads + LBBB in limb leads = Masquerading BBB, indicating advanced conduction disease.
- This pattern represents high-grade bifascicular/trifascicular block, often pre-terminal.
- In diabetics, this may reflect diffuse conduction fibrosis or ischemic conduction disease.
- Syncope/fits in such patients = high risk of complete heart block → urgent pacing required.
- Missing this diagnosis can lead to sudden cardiac death due to AV block.
👉 Key Point: “Masquerading BBB is a wolf in sheep’s clothing—pace before pause.”
🔴 Case 5: Ventricular Tachycardia with Underlying STEMI
Final Clinical Pearls:
- Wide-complex tachycardia in shock = VT until proven otherwise—never delay cardioversion.
- DC shock is life-saving and should precede detailed diagnosis in unstable patients.
- Post-cardioversion ECG may reveal underlying STEMI as the primary trigger.
- Diabetics frequently present with arrhythmia-first ACS rather than chest pain-first ACS.
- After rhythm stabilization, definitive reperfusion (PCI) remains essential.
👉 Tagline: “Shock + wide QRS = shock first, think later.”
🔴 Case 6: DCMP with Atrial Flutter and Heart Failure
Final Clinical Pearls:
- In diabetics with long-standing symptoms, DCMP with reduced EF is a common substrate for arrhythmias.
- Atrial flutter with LBBB and low EF indicates advanced electrical and mechanical remodeling.
- Tachyarrhythmia in DCMP can precipitate acute decompensated heart failure (“tachycardia-induced cardiomyopathy”).
- Rate/rhythm control + diuretics + neurohormonal blockade + SGLT2 inhibitors form the cornerstone.
- SGLT2 inhibitors (e.g., dapagliflozin) provide dual benefit—glycaemic + heart failure outcome improvement.
- Avoid indiscriminate AV nodal blockers in unstable HF—hemodynamic status guides therapy.
👉 Key Point: “In diabetes, arrhythmia is often the voice of failing myocardium.”
🔶 Grand Integrated CME INDIA Takeaways
| Electrolyte disturbances + ischemia + conduction disease frequently coexist in diabetics—never think in silos. |
| ECG in diabetes is often deceptive—look beyond classical patterns. |
| Arrhythmia, not pain, may be the first manifestation of ACS in diabetes. |
| Hyperkalaemia and renal dysfunction amplify every cardiac emergency. |
| Early recognition + parallel management (electrolytes + rhythm + reperfusion) saves lives. |
CME INDIA Tail Piece
🧠 CME INDIA Golden Principle of ECG Interpretation:
“An ECG should always be interpreted in the light of the patient’s clinical symptoms—never in isolation.” – Ary L. Goldberger, Goldberger’s Clinical Electrocardiography: A Simplified Approach
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs