

CME INDIA Case Presentation by Dr. Firdous Shaikh, (MBBS, CPS. Diab (MUM), Pg Dip. Diab (RCP UK), Pg Dip. Diab (Emory School of Medicine USA), Consultant Physician and Diabetologist, Jyoti Clinic (Bandra, Mumbai) & Apex group of Hospitals (Mumbai); Dr. N. K. Singh, Editor, CME INDIA. Commentary By Dr. Rajeev Ranjan, MD(DVL), Asso.Prof of Dermatology, JLNMC-Bhagalpur, Bihar.
CME INDIA Case Study
How Presented?
- Mr. X is a 22-year-old male who presented with a sudden onset of fever accompanied by petechial skin lesions. Past Medical History.
- Mr. X has no significant past medical or surgical history, and no known co-morbidities. His family history is unremarkable, and he reports no known drug or food allergies. He does not have any habits, such as smoking or alcohol use, and he is sexually active. Additionally, he has no recent travel history.
Timeline and Clinical Presentation
- Skin Lesion Progression from Day 1




Day 1 (24/10/2024)
- Sudden onset fever (102°F).
- Development of petechial skin lesions initially on palms.
- Progression to ecchymosis on fingers of both hands.
- No respiratory, abdominal, CNS, or genitourinary complaints.
Initial Laboratory Findings
- Fever profile: Negative.
- Complete Blood Count: Normal.
- Liver Function Tests: Normal.
- Renal Function Tests: Normal.
- Bleeding Profile: Normal.
- Total IgE: 2573.
Initial Treatment Plan
- Valacyclovir 1000 mg OD.
- Hydroxyzine (Atarax) 10 mg BD.
- Paracetamol 1g SOS for fever.
- Fexofenadine 180 mg BD.
- Pantoprazole 40 mg OD.
- Dexamethasone 4 mg BD.
- Multivitamin injection.
Day 3 (27/10/2024)
- Minimal resolution of lesions.
- Skin biopsy performed.
Day 9 (2/11/2024)
Histopathology Report:
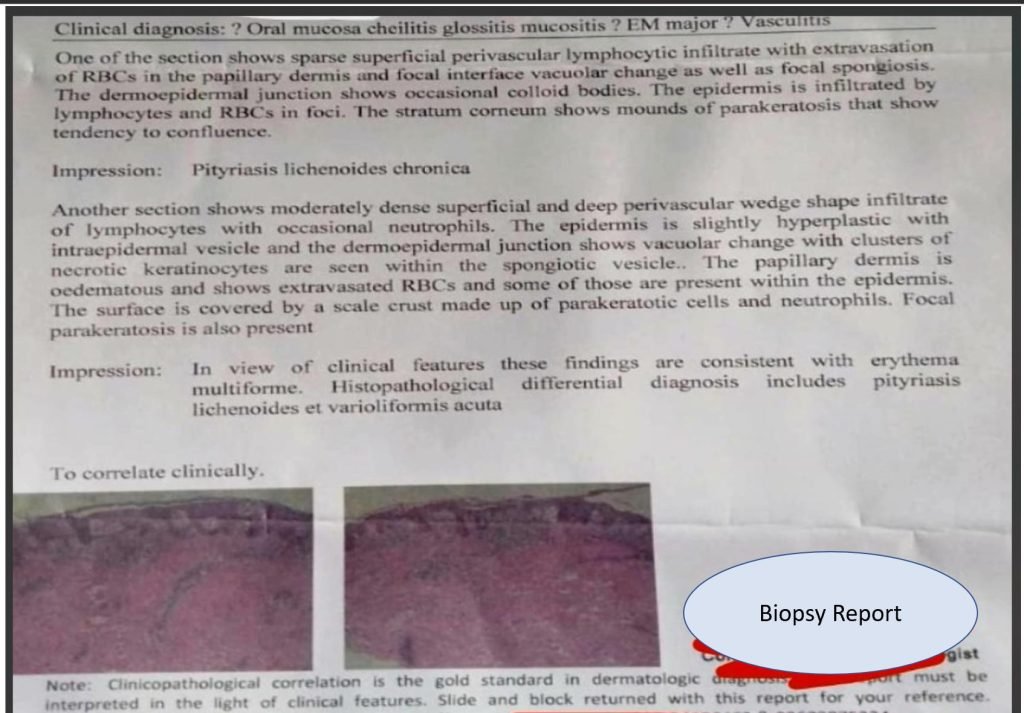
What was Primary Diagnosis?
- Erythema Multiforme.
Differential diagnosis
- Pityriasis Lichenoides et Varioliformis Acuta (PLEVA)
Day 12 (5/11/2024)
Clinical Progress:
- Mild improvement in symptoms and signs
Laboratory Investigations:
| Serum IgE: 6482 (significantly elevated from initial value) |
| Urine R&M: Normal |
| HbA1c: 5.5% |
| TSH: 5.6 |
| SGPT: 20 |
| Creatinine: 1.02 |
| Triple H Test: Negative |
| ANA: Negative |
| HSV-2 IgG: Borderline positive |
| C3, C4: Within normal limits |
Dermatology Consultation and Modified Treatment Plan
- Prednisolone 20 mg OD (after breakfast).
- Pantoprazole 40 mg OD (before breakfast).
- Sodium Pyrrolidone Carboxylic Acid (2.5%) lotion BD.
- Vitamin D 60K weekly for 8 weeks.
Discussion
This case presents a young adult male with classic features of Erythema Multiforme.
- Confirmed by histopathology. Notable findings include:
- Rapid onset of symptoms with fever and characteristic skin lesions.
- Significantly elevated IgE levels with further increase during the course.
- Borderline positive HSV-2 IgG, suggesting possible viral trigger
- Initial treatment showed minimal response, necessitating modification to systemic corticosteroids.
Take Home Points
| 1. The importance of skin biopsy in confirming diagnosis. |
| 2. The role of serial IgE monitoring in tracking disease activity. |
| 3. The necessity of dermatology consultation in cases with minimal response to initial therapy. |
| 4. The potential association between HSV infection and Erythema Multiforme. |
Commentary (Dr. Rajeev Ranjan)
- The diagnosis of the case has been labelled as Erythema Multiforme.
- There is a Prodrome of Constitutional symptoms, including Fever and others.
- This is followed by the onset of the cutaneous rash in the Acral areas and progressing Centripetally. The Lesions are probably Symmetrical, though not obviously seen in the pics provided.
- Areas involved constitute < 10% of the BSA.
- The Lesions are in different stages of evolution.
- Classical Target lesions are NOT discernible.
- Oral Mucosal lesions are present, as mentioned in the heading of the Biopsy request, though not described in the case report.
- NO involvement of Ocular, Genitourinary mucosa.
- EM Major requires 2 or more mucosae to be affected.
- Some lesions clinically appear like Vasculitis, but Biopsy reports NO Fibrin in the vessel walls and NO Thrombi in the vessel lumen, thereby Ruling out Vasculitis.
- IgE is highly elevated and increasing further in the course.
- HSV IgG is high. So, a diagnosis of Erythema Multiforme Minor may be made.
PLEVA, also known as Mucha Habermann Disease is a Differential here.
- PLEVA lesions are also sudden onset rashes.
- Progressing from Macules to Papules to Vesicles to Pustules and Erosions, Necrosis and Ulcerations may occur. Distribution here is more Axial. Trunk and Proximal Extremities, especially Flexural surfaces are mostly affected.
- Mucosal affections are uncommon. Fever, Pruritus and irritation may be present in varying degrees.
- Many viral and other infections may be the triggering agent.
- A variant of PLEVA, known as Febrile Ulceronecrotic Mucha Habermann Disease FUMHD is a very severe subtype of PLEVA, in which there are necrotic ulcers, along with CNS and other Systemic features. The prognosis is NOT v good in this type.
Stevens Johnson Syndrome SJS
- Needs to be ruled out in such cases.
- The cutaneous lesions are Erythematous Macules, Papules, Vesicular and Ulcer & Erosions.
- The Classical Target lesions are NOT present.
- The lesions are more over Face, Truncal, Proximal > Distal, and involvement is < 10% BSA.
- Oral and other mucosae are involved with Blisters, Erosions and Crusts.
- Fever, Malaise, Body ache, and Other Constitutional Symptoms are present.
- General condition is poor.
- Mostly caused by some Medication.
- It’s a more serious condition and needs Hospitalisation and Intensive care.
CME INDIA Highlights
This case involves a young adult male presenting with classical features of Erythema Multiforme (EM), confirmed via histopathology. The key clinical findings and course of the disease highlight both diagnostic challenges and management strategies:
- The patient exhibited an acute onset of fever accompanied by characteristic skin lesions. These findings align with the prodromal phase seen in EM, marked by constitutional symptoms preceding the skin eruptions.
- Serial IgE monitoring revealed highly elevated levels that increased during the disease course, suggesting an inflammatory or hypersensitivity-driven process.
- While the association between herpes simplex virus (HSV) and EM is well-documented, a borderline positive HSV-2 IgG points to a potential viral trigger for this episode. This aligns with studies identifying HSV infections, especially HSV-1, as a frequent precipitant of EM
- Initial management showed limited response, necessitating systemic corticosteroids, which led to symptom control. This underscores the importance of flexible treatment approaches based on disease severity and response.
- Histopathology is critical for diagnosing EM and ruling out differentials like vasculitis or Stevens-Johnson Syndrome (SJS).
- Serial IgE levels may serve as a marker for disease activity, although further research is needed to standardize its application.
- Cases with limited response to initial therapy should involve dermatology specialists for advanced management and differential diagnosis.
- The documented link between HSV infection and EM emphasizes the need to investigate possible viral triggers in similar presentations.
- As per Dr Rajeev commentary, the diagnosis of Erythema Multiforme Minor is supported by the histopathological findings, clinical features, and lack of systemic mucosal involvement typical of EM Major. The prodrome of fever and constitutional symptoms followed by acrally distributed cutaneous lesions progressing centripetally is characteristic.
- While classical target lesions are absent, the biopsy confirms EM rather than vasculitis (no fibrin or thrombi). Oral mucosal involvement was noted but not described in detail.
Differential Diagnoses:
- PLEVA (Much Habermann Disease): Sudden onset of rashes progressing from macules to necrotic ulcers, typically involving the trunk and proximal extremities, must be differentiated. The absence of severe systemic involvement and axial distribution rules against PLEVA or its severe variant, Febrile Ulceronecrotic Mucha Habermann Disease (FUMHD).
- SJS: Although SJS and EM share overlapping features, SJS often involves medication as a trigger, systemic mucosal involvement, and poorer prognosis. The distribution and lack of extensive BSA involvement (<10%) in this case argue against SJS.
References:
- Susanto, Hendri & Nurhilailah, Nurhilailah & Ganesha, Raziv & Hendarti, Hening & Hadi, Priyo. (2022). Herpes-associated erythema multiforme in a postmenopausal woman. Majalah Kedokteran Gigi Indonesia. 7. 51. 10.22146/majkedgiind.43299.
- Wetter DA, Davis MDP. Recurrent erythema multiforme: clinical characteristics, etiologic associations, and treatment in a series of 48 patients at Mayo Clinic, 2000 to 2007. J Am Acad Dermatol. 2010 Jan;62(1):45-53. doi: 10.1016/j.jaad.2009.06.046. Epub 2009 Aug 7. PMID: 19665257.
- Soares, A.; Sokumbi, O. Recent Updates in the Treatment of Erythema Multiforme. Medicina 2021, 57, 921. https://doi.org/10.3390/medicina57090921
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
I want latest updates in cardiology