

CME INDIA Presentation by Dr. Mahendra Nawaria, President of the All India Association for Advancing Research in Obesity (AIAARO) , Director , Asian Bariatrics Private Limited and Chairman, AB Plus Super Speciality Hospital, Thaltej–SG Highway, Ahmedabad, Gujarat & Dr. Banshi Saboo, Chair, International Diabetes Federation (IDF), South-East Asia Region ,Chief Diabetologist & Chairman, Diabetes Care & Hormone Clinic (DiaCare), Ahmedabad.
Body Mass Index (BMI) is commonly used to classify obesity, but it does not fully account for variations in body composition and fat distribution. This is particularly evident in South Asians, who display unique patterns of adiposity even at lower BMI thresholds. A closer examination reveals that individuals within this population, despite having similar BMI, can exhibit significantly different levels of visceral fat. These disparities are influenced by a combination of genetic factors and early nutritional experiences.
Look This Picture Carefully
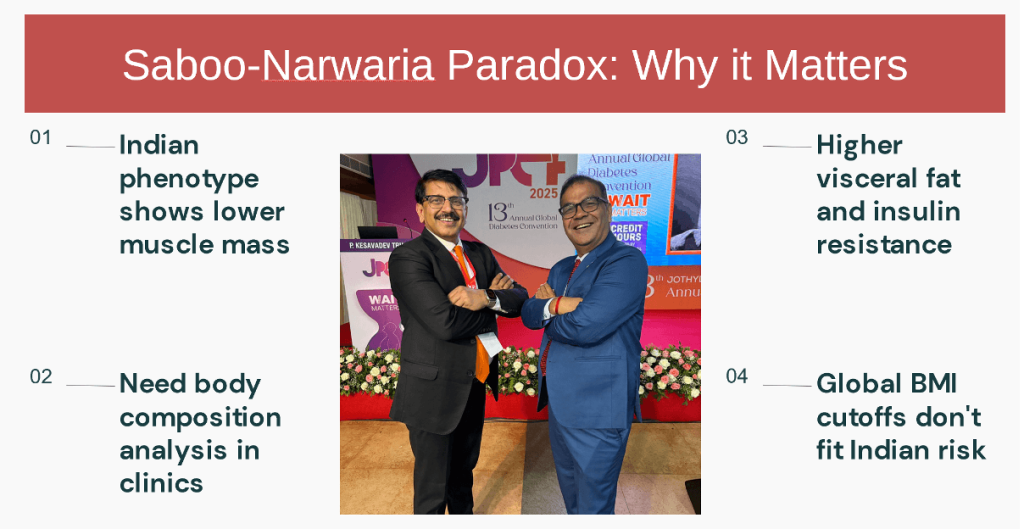
- At the Jothydev’s Professional Education Forum (JPEF) 2025, the “Saboo-Nawaria Paradox” was presented, highlighting two eminent doctors with differing body composition despite relatively close BMI values.
- Obesity is traditionally defined by Body Mass Index (BMI), a convenient anthropometric index correlating weight with height. However, BMI neither differentiates fat from lean mass nor provides insight into fat distribution, limiting its utility as a predictor of cardiometabolic risk.
- This limitation is particularly problematic in South Asians, where the phenotype is characterized by lower BMI but increased central adiposity and visceral fat accumulation — the so-called “thin-fat” Indian paradox.

Objective:
We describe the “Saboo-Nawaria Paradox,” where two individuals of similar ethnic background exhibit divergent body composition despite comparable BMI, highlighting why BMI alone is insufficient for assessing obesity and cardiometabolic risk.
Methods:
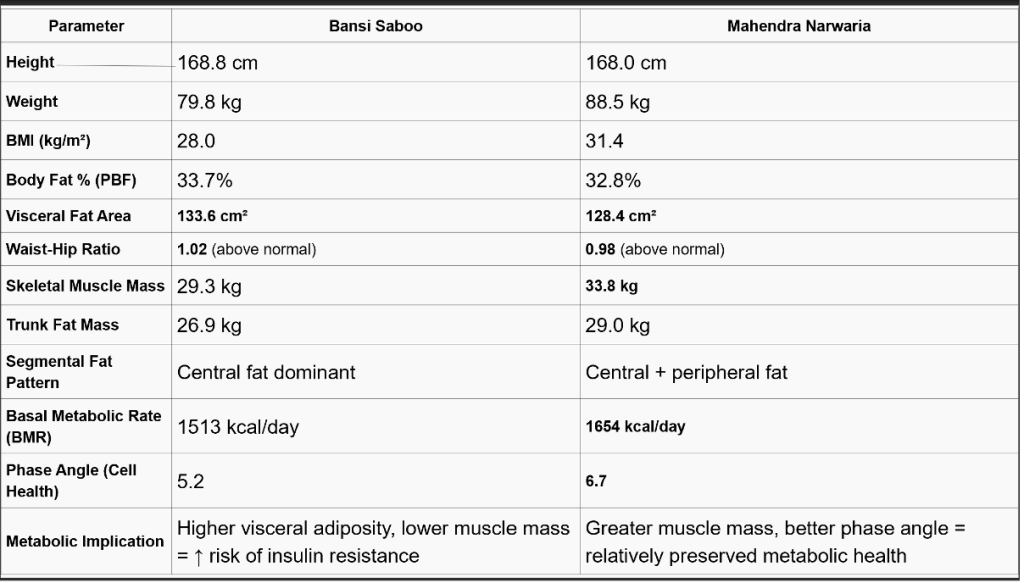
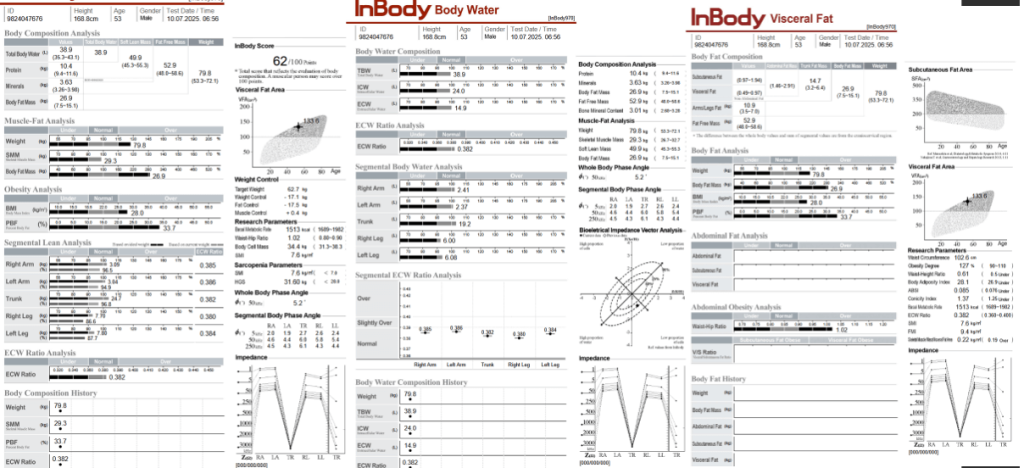
Comparative body composition analysis of two Indian diabetologists, Dr. Banshi Saboo and Dr. Mahendra Narwaria, was presented at the 13th Annual Global Diabetes Convention (JPEF 2025). Parameters included BMI, body fat percentage, visceral fat area (VFA), waist-hip ratio (WHR), skeletal muscle mass, fat distribution, and basal metabolic rate (BMR).
Results:
- Despite having a lower BMI (28.0 kg/m² vs 31.4 kg/m²), Dr. Saboo had a higher visceral fat area (133.6 cm² vs 128.4 cm²) and unfavorable waist-hip ratio (1.02 vs 0.98) compared to Dr. Narwaria, whose higher BMI reflected greater skeletal muscle mass (33.8 kg vs 29.3 kg).
- Dr. Saboo demonstrated a central fat-dominant pattern with lower muscle mass, suggesting a higher cardiometabolic risk profile, whereas Dr. Narwaria’s profile was relatively metabolically healthier despite a higher BMI.
Conclusion:
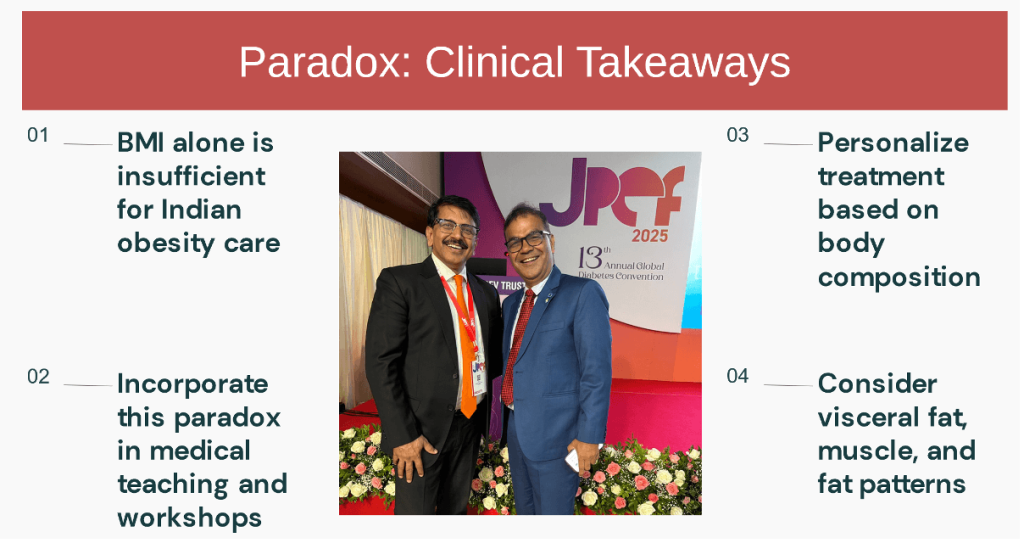
- The Saboo-Nawaria Paradox underscores a key limitation of BMI in diagnosing obesity among South Asians. BMI does not distinguish between fat and lean mass nor reflect visceral adiposity, the critical determinant of cardiometabolic risk.
- Clinicians should incorporate additional measures such as waist circumference, WHR, visceral fat area, and skeletal muscle mass when assessing obesity, particularly in populations prone to central obesity at lower BMIs.
What this Paradox teaches us?
- While BMI suggested that Dr. Narwaria was more obese, Dr. Saboo exhibited greater visceral adiposity and a higher waist-hip ratio, both stronger predictors of diabetes and cardiovascular disease.
- The differences observed illustrate fundamental weaknesses of BMI:
- Body composition: BMI cannot distinguish between adipose tissue and lean mass. A higher BMI may reflect increased muscle rather than excess fat.
- Visceral vs. subcutaneous fat: Visceral fat correlates more strongly with cardiometabolic risk than subcutaneous fat, but BMI fails to capture this.
- Ethnic variability: South Asians accumulate visceral fat at lower BMI thresholds, necessitating revised diagnostic criteria and more sensitive tools.
- Emerging data consistently demonstrate that waist circumference, waist-hip ratio, and direct measures of visceral fat area provide superior risk stratification, particularly for South Asians.
Clinical Implications:
| The differences observed illustrate fundamental weaknesses of BMI: |
| Body composition: BMI cannot distinguish between adipose tissue and lean mass. A higher BMI may reflect increased muscle rather than excess fat. |
| Visceral vs. subcutaneous fat: Visceral fat correlates more strongly with cardiometabolic risk than subcutaneous fat, but BMI fails to capture this. |
| Ethnic variability: South Asians accumulate visceral fat at lower BMI thresholds, necessitating revised diagnostic criteria and more sensitive tools. |
| Emerging data consistently demonstrate that waist circumference, waist-hip ratio, and direct measures of visceral fat area provide superior risk stratification, particularly for South Asians. |
CME INDIA Learning Points
| The “Saboo-Nawaria Paradox” provides a compelling real-world example of BMI’s limitations. |
| A comprehensive approach to obesity assessment, incorporating anthropometry, body composition, and fat distribution markers, is essential for accurate risk stratification and personalized management, especially in South Asians. |
| BMI does not capture body composition or visceral adiposity. |
| South Asians have greater central adiposity even at lower BMIs. |
| Waist circumference, WHR, visceral fat estimation, and muscle mass assessments must complement BMI in clinical practice. |
CME INDIA Tail-Piece
Liten to Dr. Banshi Saboo and Dr. Mahendra Nawaria – What’s remedy, why it happened?
References:
- Misra A, Shrivastava U. “South Asians tend to accumulate more tummy fat even at lower weight — this ‘thin-fat’ Indian type explains why BMI may not work properly for us.” Indian J Endocrinol Metab. 2013;17(5):667–675. doi:10.4103/2230-8210.117212
- WHO Expert Consultation. “For Asian people, health risk starts at a lower BMI, so BMI cut-offs for overweight and obesity need to be lowered for us.” Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
- Lear SA, Humphries KH, Kohli S, Birmingham CL. “Even when BMI is low, Indian-origin persons may have fat around organs (visceral fat), not visible from outside but risky for diabetes.” Int J Obes (Lond). 2007;31(3):555–560. doi:10.1038/sj.ijo.0803433
- Yajnik CS, Yudkin JS. “This concept of ‘thin-fat’ Indian shows that body fat percentage and where fat is located matter more than just weight and height.” Eur J Clin Nutr. 2004;58(7):787–793. doi:10.1038/sj.ejcn.1601925
- Vaidya V, Paradkar A, Joshi S. “Visceral adiposity, not just weight, predicts diabetes in urban Indian adults — and BMI alone misses this silent fat.” J Assoc Physicians India. 2021;69(7):34–38. JAPI
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
It was pondered, long ago about this idea. But in practice it was difficult to draw results and conclusions for estimation. MRI is the way out to determine. Now of late some gadgets have come into vogue. This will give the exact risk assessment.
The YY paradox of YAGINIC,was well appreciated long ago. Now the old wine in a new bottle with DR SABOO and NAVARIA, depicts the present reality. Dr Saboo is well known for his simplicity talk which is admired globally. Good eye opener.