
CME INDIA Presentation by Dr. N. K. Singh, Diabetes Care Physician, Dhanbad, Editor-in Chief, CME INDIA.
Based on a presentation at Diacarecon, Ahmedabad, 2025.


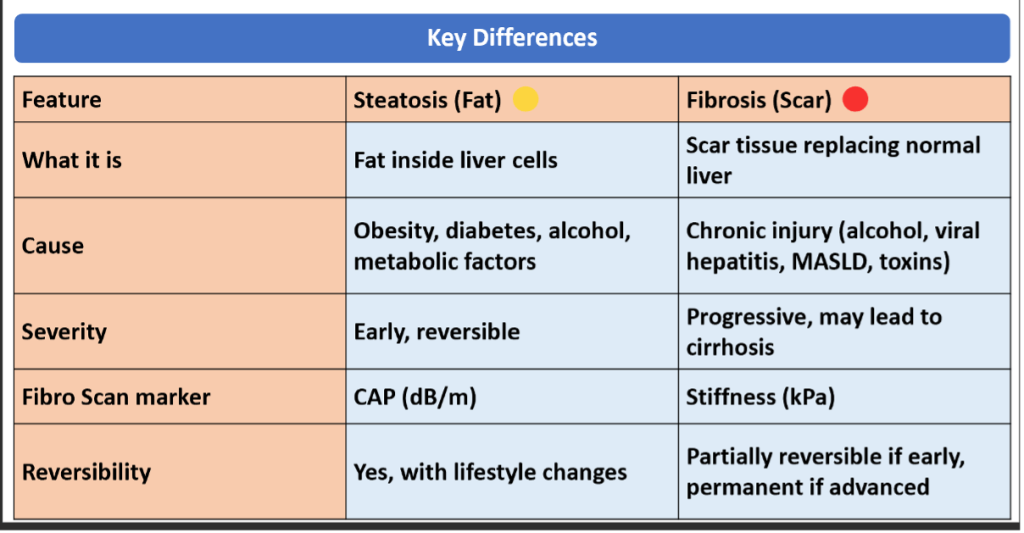
What is Steatosis (Fatty Liver)
| Definition: Accumulation of fat (triglycerides) inside liver cells (hepatocytes). |
| Cause: Commonly due to obesity, diabetes, alcohol, high cholesterol, certain drugs, or metabolic dysfunction–associated steatotic liver disease (MASLD, previously NAFLD). |
| Reversibility: Yes – if lifestyle changes are made (weight loss, exercise, diet, stopping alcohol). |
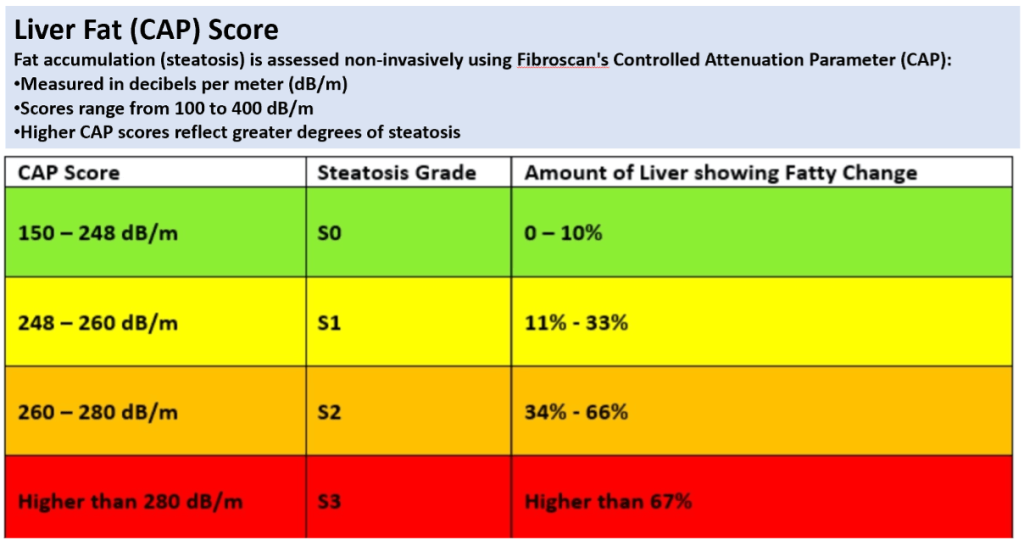
| Measured by FibroScan CAP (Controlled Attenuation Parameter): |
| S0: <238 dB/m → no steatosis |
| S1: 238–260 → mild |
| S2: 260–290 → moderate |
| S3: >290 → severe |
| Think of steatosis as “fat in the liver” – the earliest change. |
Fibrosis (Scarring of Liver)
| Definition: Formation of scar tissue in the liver due to chronic injury (alcohol, hepatitis, MASLD, toxins). |
| Mechanism: The liver tries to repair damage, but repeated injury leads to collagen deposition and scarring. |
| Reversibility: Early fibrosis (F1–F2) may be partly reversible; advanced fibrosis and cirrhosis (F3–F4) are harder to reverse. |
| Measured by FibroScan stiffness (kPa): |
| F0: <6 kPa → no fibrosis |
| F1: 6–7 kPa → mild fibrosis |
| F2: 7–9 kPa → significant fibrosis |
| F3: 9–12 kPa → advanced fibrosis |
| F4: >12–14 kPa → cirrhosis |
| Think of fibrosis as “scar tissue in the liver” – more serious than steatosis |
Knowing this is Important
What is Transient Elastography (TE)
| A technique that uses a vibration pulse and ultrasound waves to measure liver stiffness. |
| Principle: A mechanical vibration generates a shear wave through the liver, and ultrasound measures how fast the wave travels. Faster wave = stiffer liver (fibrosis). |
| Output: Stiffness in kilopascals (kPa) and often CAP score (dB/m) for fat. Use: Detects fibrosis and steatosis in a non-invasive, painless way. It’s a method, not a machine. |
What is FibroScan?
| A specific device/brand (by Echosens, France) that performs transient elastography. |
| It is the most widely used machine for TE in liver disease. |
| Provides: LSM (liver stiffness measurement, kPa) → fibrosis |
| CAP (controlled attenuation parameter, dB/m) → steatosis |
| Other companies also make TE machines, but FibroScan is the original and most validated |
History of FibroScan (TE)
- Early Concept (1990s)
- Traditional liver biopsy was the gold standard for fibrosis, but it was invasive, painful, and had sampling errors.
- Researchers in France began exploring non-invasive methods based on ultrasound elastography to measure liver stiffness.
- Development Phase (Late 1990s – Early 2000s)
- The principle of transient elastography was developed: low-frequency vibrations generate shear waves, and ultrasound tracks their velocity to calculate tissue stiffness.
- Early prototypes were tested at Pitié-Salpêtrière Hospital, Paris.
- First Commercial Launch (2003)
- FibroScan (by Echosens, France) became the first commercial transient elastography device.
- Initially validated in chronic hepatitis C, showing high accuracy in detecting advanced fibrosis and cirrhosis.
- Global Expansion (2005–2015)
- Rapid adoption in Europe and Asia, later in the US (FDA approval in 2013).
- Applications expanded from viral hepatitis to MASLD (NAFLD/NASH), alcoholic liver disease, autoimmune hepatitis, and cholestatic disorders.
- Addition of Controlled Attenuation Parameter (CAP) in 2010 allowed simultaneous assessment of steatosis.
- Recent Advances (2016–Present)
- Broader use in primary care, endocrinology, and diabetes clinics for MASLD screening.
- Development of XL probe for obese patients and M+ probe for pediatrics.
- Incorporated into guidelines (AASLD, EASL, APASL) as a first-line tool for fibrosis risk stratification.
- Current research explores combination with biomarkers (Fib-4, ELF, FAST score) for precision diagnosis and monitoring

Key Differences at a Glance
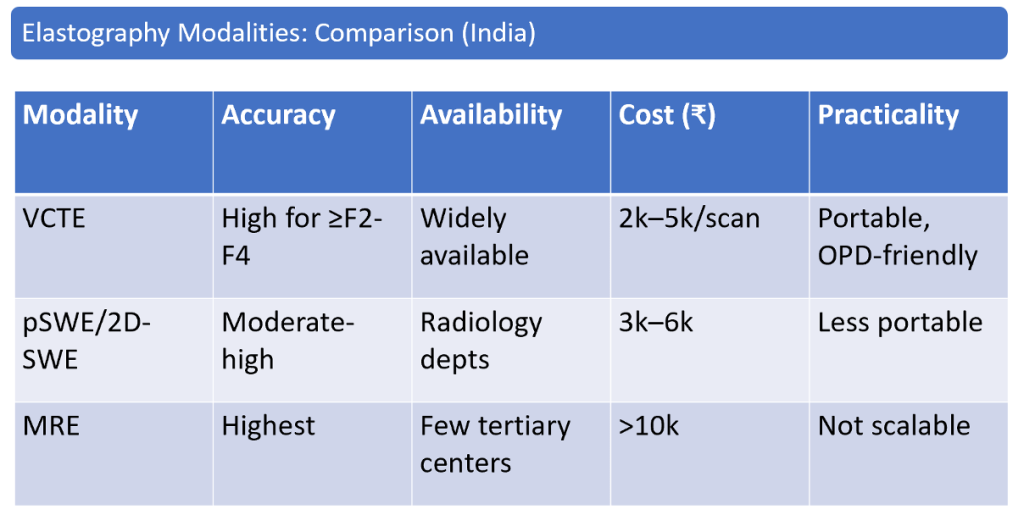
- TE (FibroScan): Portable, fast, screening tool, validated cut-offs, but blind and limited in ascites/obesity.
- SWE: US-guided, detailed elastogram, works in ascites/obesity, more versatile, but less standardized and needs US expertise.
- Use *FibroScan (TE) when you want quick, standardized fibrosis/steatosis staging in large populations.
- Use SWE when you need precise, US-guided, focal liver assessment or in difficult patients (ascites, obesity, lesions).
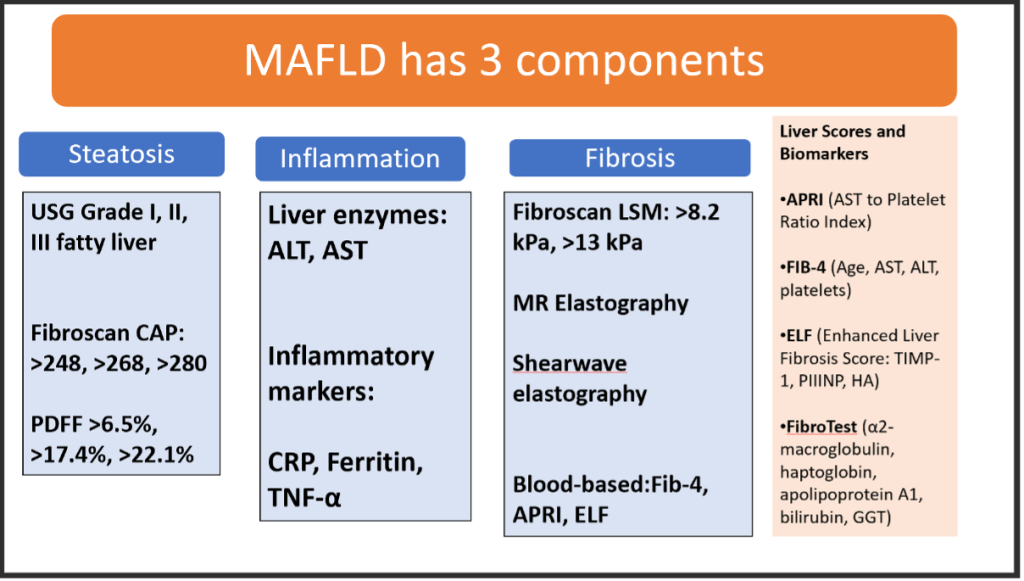
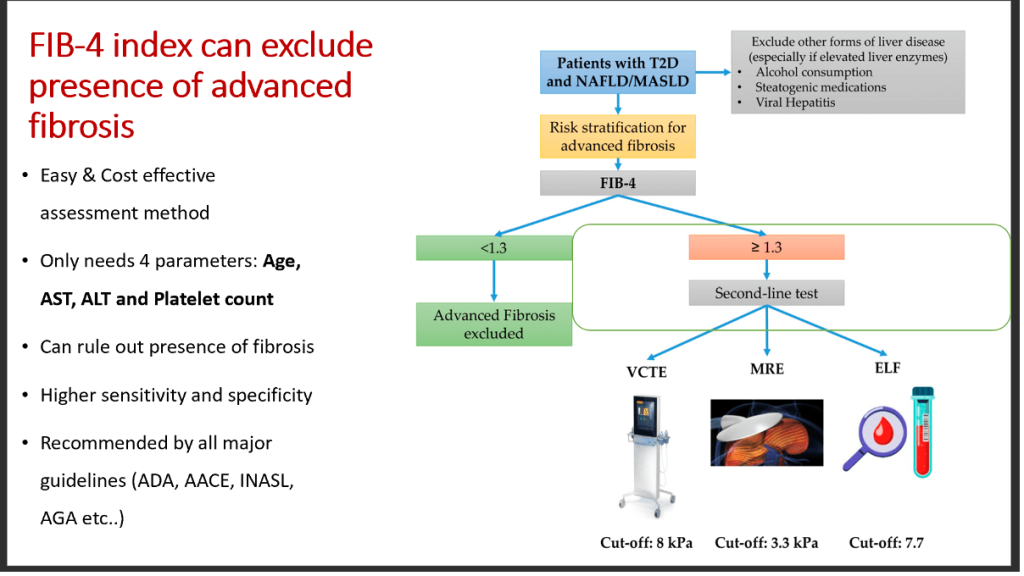
Fib-4 is the New Mantra in Diabetes Care

When you get a report of Fibro scan, what to see?
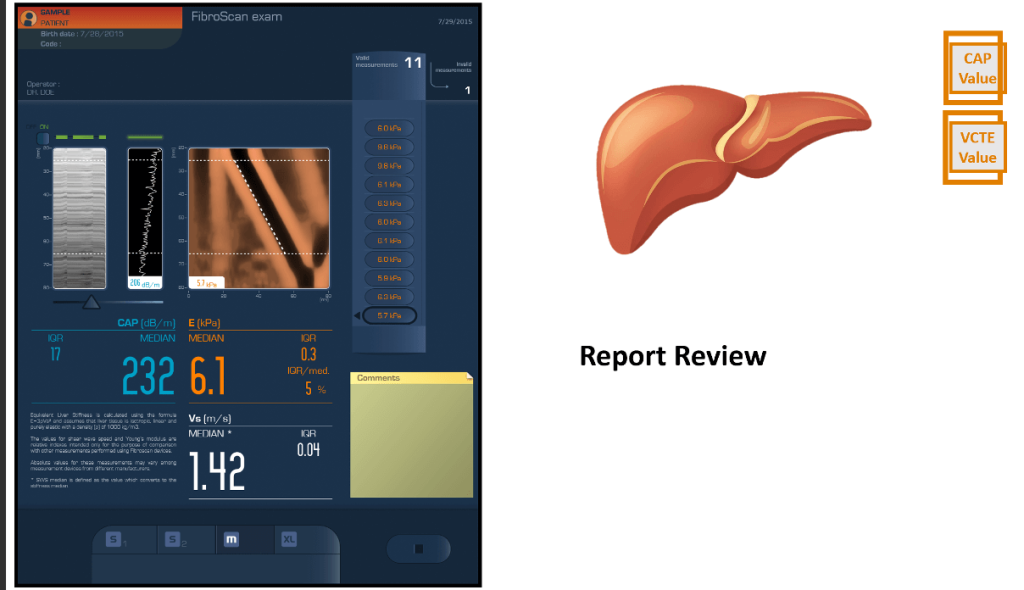
This report shows:
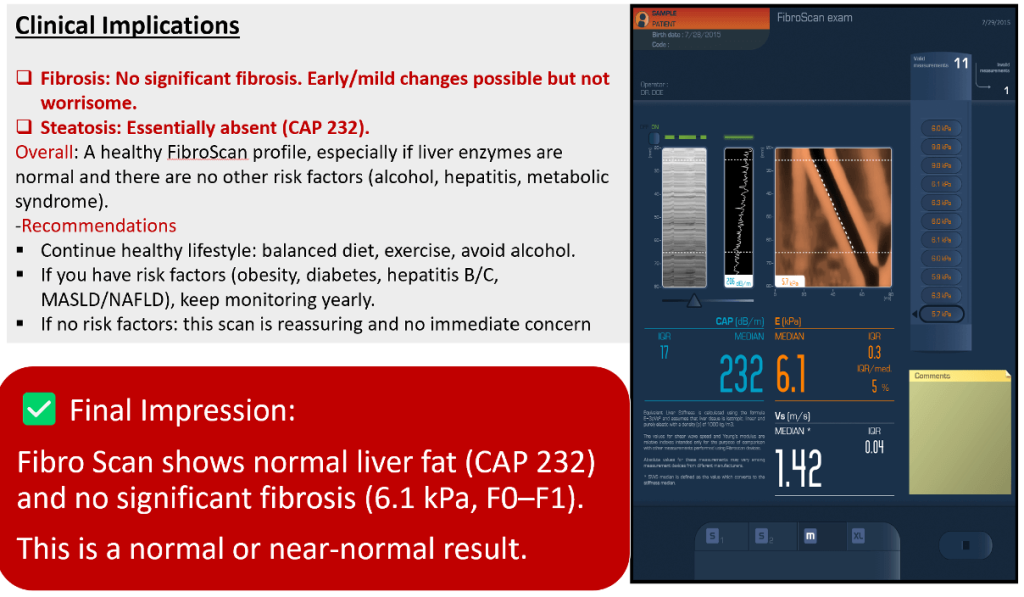
- Median Liver Stiffness (E): 6.1 kPaI
- QR: 0.3 kPa →
- IQR/Median ratio: 5% (very reliable, <30% acceptable)Valid
- Measurements: 11 (meets quality criteria, ≥10 required)
- Shear Wave Speed (Vs): 1.42 m/sCAP
- (Controlled Attenuation Parameter): 232 dB/m (measures liver fat)
Interpretation
| Fibrosis (Stiffness) |
| Normal liver: ~2.5–5.5 kPa |
| Borderline zone: 5.5–7 kPa → may indicate early fibrosis (F1–F2), depending on context |
| Significant fibrosis (≥F2): >7–8 kPa |
| Cirrhosis (F4): >12–14 kPa➡ Your result: 6.1 kPa |
This report:
| 6.1 kPa |
| Slightly above normal but below the threshold for significant fibrosis. |
| Consistent with F0–F1 (no to mild fibrosis). |
Next to See:
Steatosis (Fat in Liver, CAP Score)
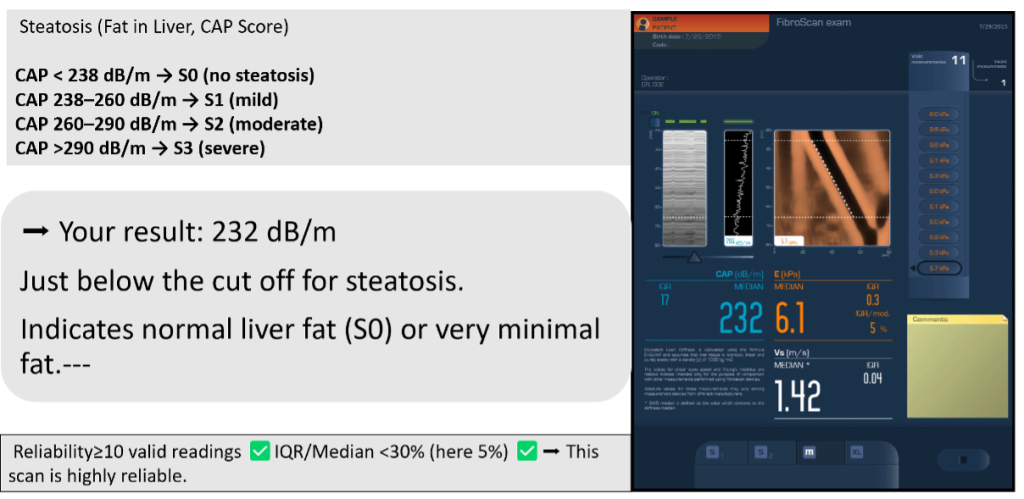
Final Impression:
Another Case
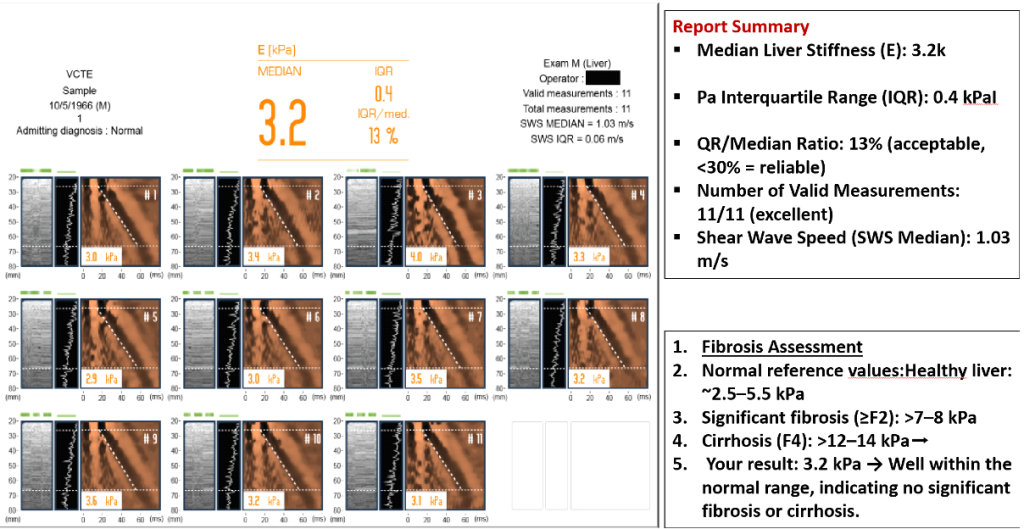
Reliability of Scan
- At least 10 valid readings required → You have 11.
- IQR/Median <30% →
- Your ratio is 13%, so results are highly reliable.
- Clinical Implications
- Liver stiffness is normal.
- Suggests absence of advanced liver disease (fibrosis/cirrhosis).
- If liver enzymes (ALT, AST) are normal and there are no risk factors (alcohol, viral hepatitis, metabolic syndrome, MASLD/NAFLD), this scan is reassuring.
- Recommendations:
- Maintain healthy lifestyle: balanced diet, avoid excess alcohol, maintain healthy weight.
- If you have risk factors (diabetes, obesity, viral hepatitis, fatty liver), continue routine follow-up with liver function tests and periodic scans. Otherwise, no evidence of chronic liver damage at present.
- Final Impression: FibroScan is normal (3.2 kPa), no evidence of significant fibrosis or cirrhosis.
What the Clinician needs to know?

CME INDIA Take Away Points
1. Understand the Two Key Outputs: LSM & CAP
FibroScan provides:
- Liver Stiffness Measurement (LSM, kPa) → estimates fibrosis
- Controlled Attenuation Parameter (CAP, dB/m) → estimates steatosis
Both must be interpreted together, not in isolation.
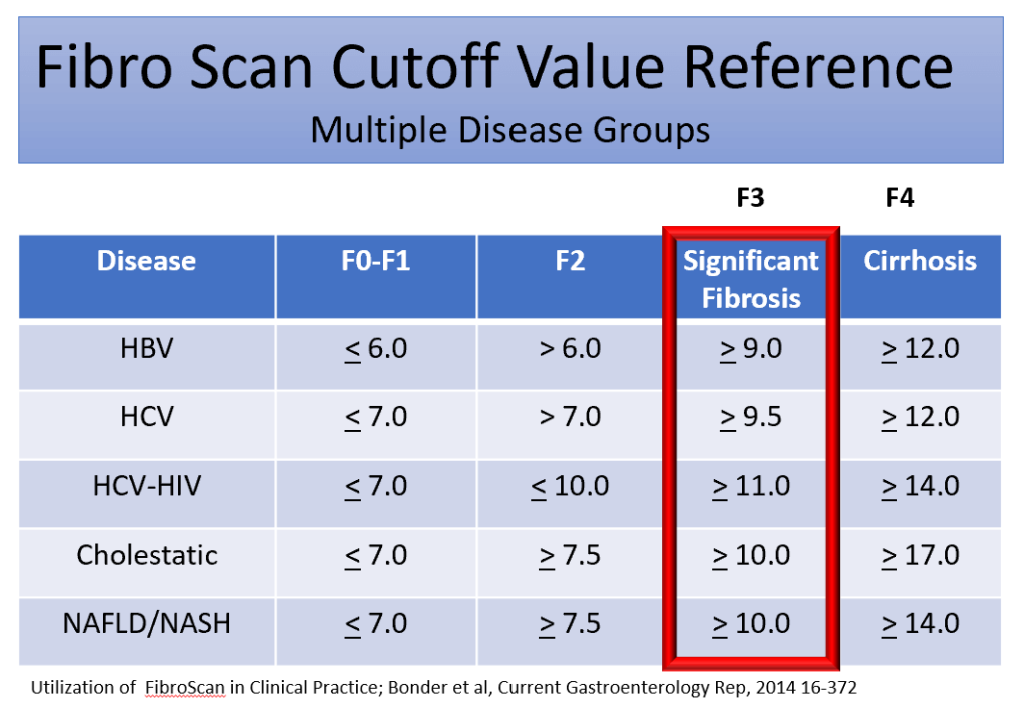
2. LSM Values Reflect Fibrosis Stage (Approximate Cut-offs)
Typical thresholds (MASLD context):
- <7 kPa → F0–F1 (Low risk)
- 7–9 kPa → F2 (Intermediate risk)
- ≥10 kPa → F3–F4 (High risk / advanced fibrosis)
- ≥12–14 kPa → suggestive of cirrhosis
These are not absolute; integrate with clinical context.
3. CAP Score Reflects Fat Content (Steatosis Grading)
Typical CAP cut-offs:
- S1 (mild): 248–267 dB/m
- S2 (moderate): 268–279 dB/m
- S3 (severe): ≥280 dB/m
Useful for diagnosis of MASLD in diabetes.
4. FIB-4 Should Always Be Checked Before FibroScan
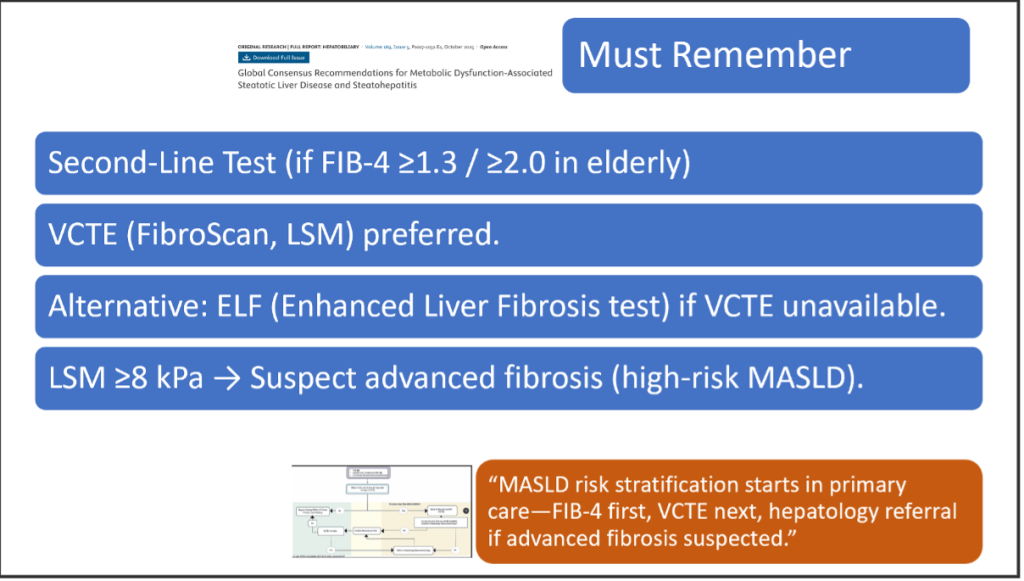
If FIB-4 >1.3 (age <65) or >2.0 (age >65) → proceed to FibroScan.
Combining FIB-4 + FibroScan improves accuracy and reduces unnecessary referrals.
5. Interpreting Results in Obesity Requires Caution
Obesity (BMI ≥30 kg/m²) can:
- Artificially increase LSM
- Reduce CAP accuracy
- Require XL probe instead of M-probe
If incorrect probe used → unreliable values.
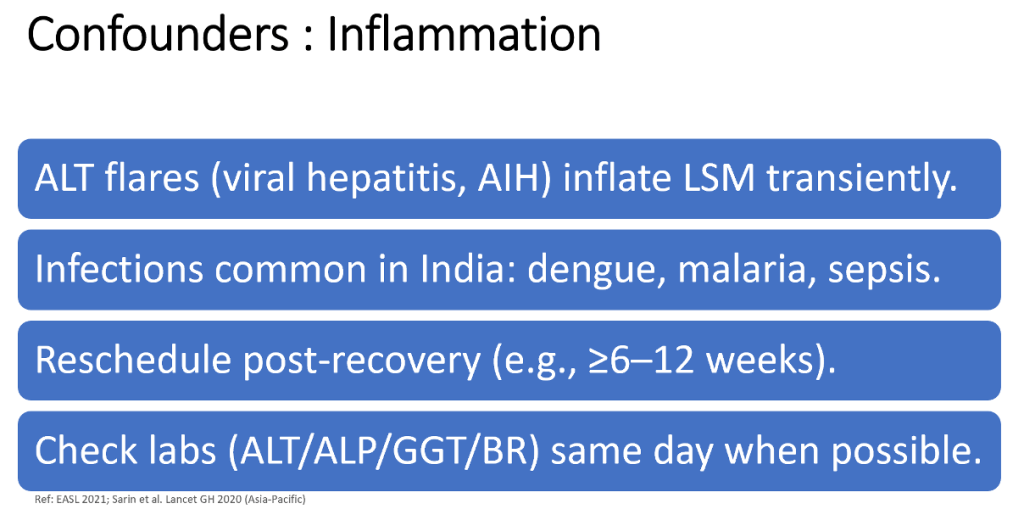
6. Inflammation, Cholestasis, or Congestive Heart Failure Can Falsely Elevate LSM
LSM increases with:
- Acute hepatitis (ALT >100–200 IU/L)
- Cholestasis / biliary obstruction
- Severe hepatic congestion (heart failure)
In these cases, repeat FibroScan after resolution.
7. Adequate Fasting Is Essential
Patients should be:
- Fast ≥3-4 hours
Food intake increases liver blood flow → false high LSM.
8. Reliability Criteria Must Be Met
A FibroScan is reliable when:
- ≥10 valid measurements
- IQR/median ≤30% for LSM
- Success rate >60%
If criteria not met → repeat test or use alternative modality.
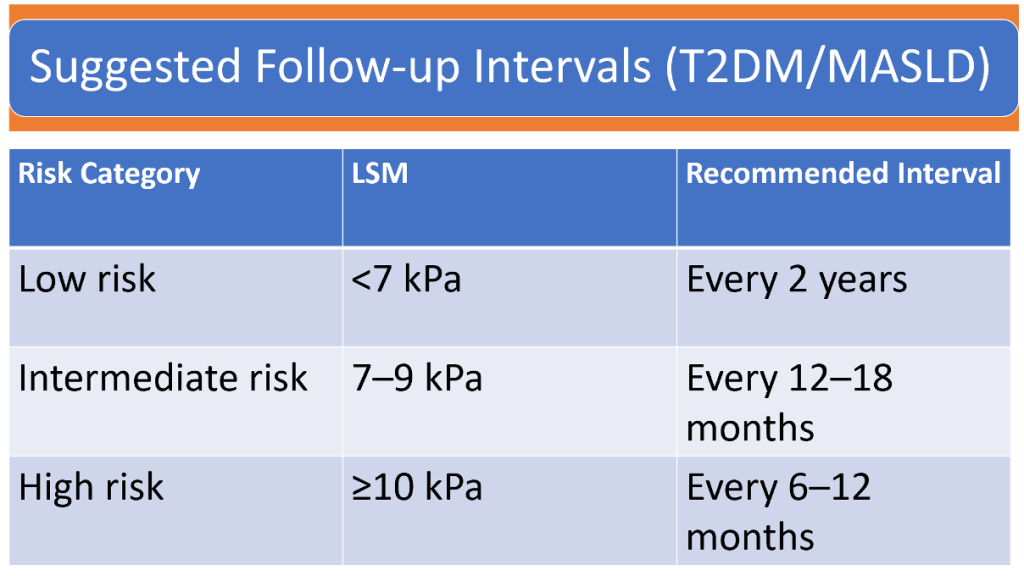
9. Follow-up Intervals Based on LSM (as in your table)
- Low risk (<7 kPa): repeat every 2 years
- Intermediate risk (7–9 kPa): every 12–18 months
- High risk (≥10 kPa): every 6–12 months
Patients with cirrhosis require:
- 6-monthly US for HCC
- Variceal screening
10. Interpretation Must Be Integrated Clinically, Not Used Alone
FibroScan does not replace:
- Liver biopsy in complex cases
- Assessment of comorbidities (diabetes, obesity, dyslipidemia)
- Evaluation of alcohol intake, medications, viral hepatitis
Always interpret with:
- ALT, AST
- Platelet count
- Metabolic profile
- Imaging
- Fibrosis scores (fib-4, nfs)
Bonus (Important for Diabetes Clinics):
- Diabetic patients have a 2–3× higher prevalence of advanced fibrosis even with normal ALT.
- FibroScan should be routinely considered in T2DM + obesity + elevated FIB-4.
CME INDIA Tail-Piece
Suggested Readings:
- American Diabetes Association. (2025). Metabolic dysfunction-associated steatotic liver disease: Consensus report and clinical recommendations. Diabetes Care, 48(7), 1057–1076. https://doi.org/10.2337/dc25-xxxx
- Zhang, Y., Liu, H., Chen, Q., & Wang, L. (2025). Liver elastography for liver fibrosis stratification: Updated evidence and clinical utility. Biomedicines, 13(1), 138. https://doi.org/10.3390/biomedicines13010138
- Patel, R., Wong, V. W., Rinella, M., & Yilmaz, Y. (2025). Staging liver fibrosis and cirrhosis using non-invasive tests: Updated systematic review and meta-analysis. Liver Research, 12(2), 134–149. https://doi.org/10.1016/j.livres.2024.11.004
- Li, X., Zhou, S., Chen, Y., & Huang, J. (2025). The accuracy of FibroScan, FIB-4, and NAFLD fibrosis score in patients with type 2 diabetes mellitus. Medicine, 104(25), e35123. https://doi.org/10.1097/MD.0000000000035123
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Very useful, informative and very practical information with fibroscan interpretation article.
A comprehensive knowledge of Fibroscsn for a learner like
Please advise when minimum fat content in liver and stiffness score was 21 now came down to 18 after 6 months.
Please advise.