
CME INDIA Presentation by Dr. Lily Rodrigues, Consultant Physician & Diabetologist at Stride Hospitals,Professor of Medicine, Maheshwara Medical College, Hyderabad.
Hyperglycemia Impacts Two Lives
- Diagnosis of GDM identifies women at high risk of future diabetes and associated metabolic problems
- Diagnosis of GDM identifies women at high risk of future diabetes and associated metabolic problems
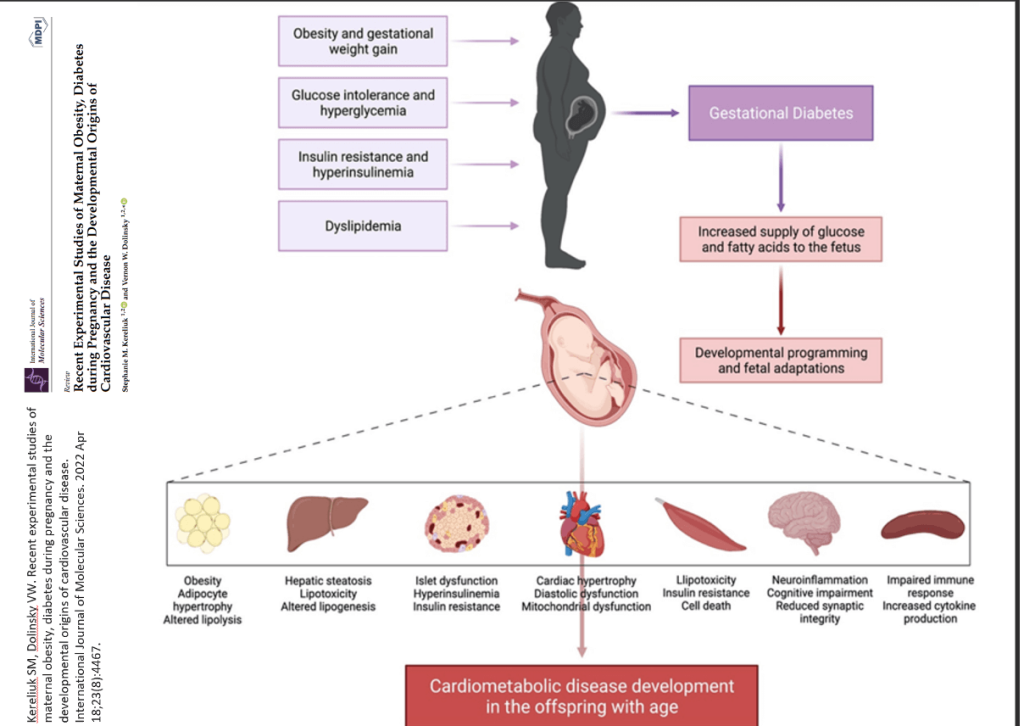
- Maternal Hyperglycemia is associated with development of metabolic problems in offsprings
Global GDM Prevalence:
- Affects approximately 13.4% of pregnancies globally (around~17 million pregnancies/year).
- Increases the risk of type 2 diabetes and other health complications for both mother and child.
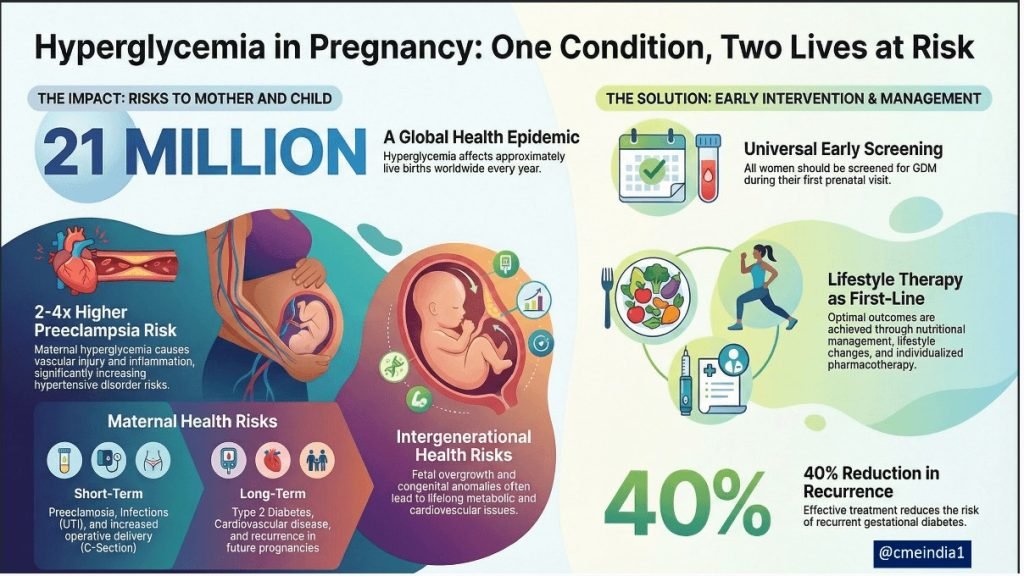
HIP is an epidemic & a global burden
- Hyperglycemia in pregnancy affects about 1 in 6 live births worldwide (~21 million per year).
- This includes pre-existing diabetes (Overt diabetes or PGDM) and gestational diabetes (GDM).
- Poorly controlled blood glucose during pregnancy increases the risk of complications both at birth and long-term for the mother and baby.
- The WHO (2025) is actively developing updated evidence-based recommendations for monitoring and management of hyperglycaemia in pregnancy to improve global maternal and new-born outcomes, especially in low- and middle-income countries.
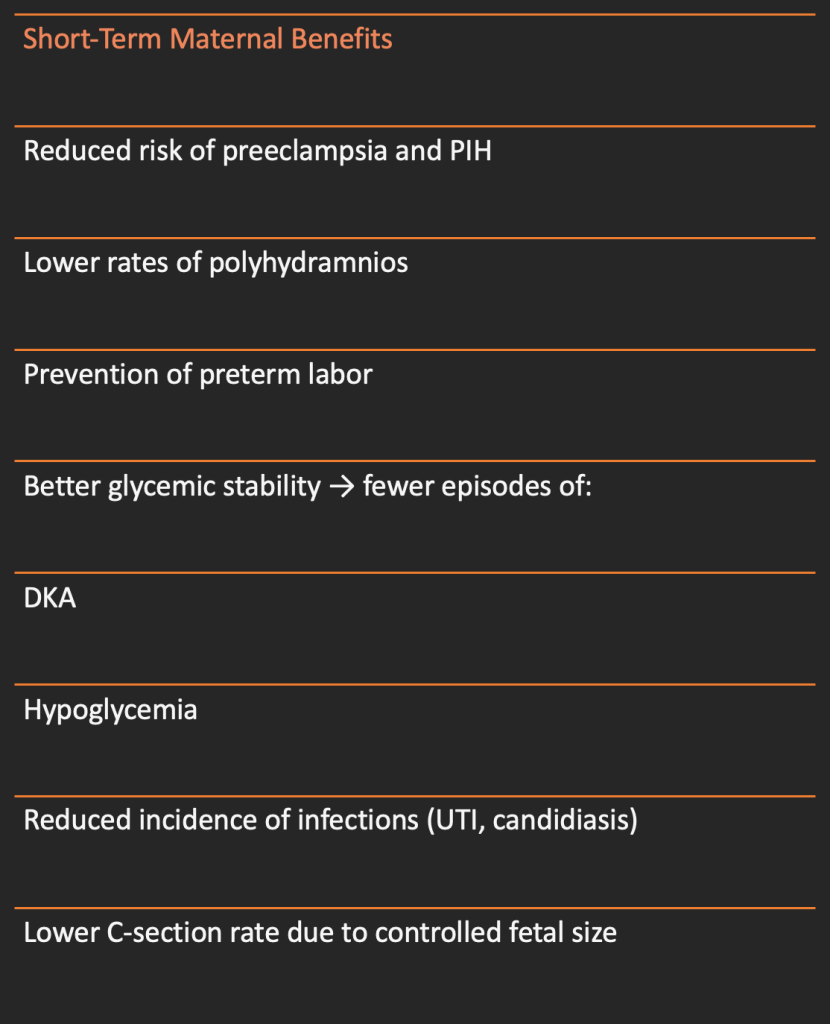
Short term Maternal Outcomes
1. Preeclampsia/Pregnancy induced hypertension
Women with Hyperglycemia have 2-4X higher risk of Hypertensive disorders of pregnancy due to;
A. Endothelial Dysfunction (because of oxidative stress, inflammation and vascular injury
- Damaged endothelium leads to: increased vascular permeability, Vasoconstriction and hypertension
B. Placental abnormalities: DM causes abnormal trophoblastic invasion-shallow placentation and thus reduced perfusion.
- Hypoperfusion triggers release of antiangiogenic factors (sFlt-1, endothelin) ultimately leading to preeclampsia
C. Insulin resistance and metabolic syndrome
- High BMI, dyslipidemia and IR all common in GDM enhance the risk of hypertension
D. Co-existing Chronic Hypertension;
- Many types 2 DM mothers also have hypertension additive risk of superimposed preeclampsia
| Types of Hypertensive Disorders in Pregnancy |
| A. Pregnancy induced Hypertension (PIH)/Gestation Hypertension |
| BP>140/90mm after 20 weeks, no proteinuria |
| Usually mild but can progress to preeclampsia |
| B. Preeclampsia; |
| Occurs after 20 weeks and includes-bp.140/90, + one or more of the following: |
| Proteinuria, >300mg/24hours, Urine PCR>0.3 |
| End organ dysfunction |
| Elevated liver enzymes, thrombocytopenia |
| Renal insufficiency |
| Pulmonary edema, visual disturbance |
| OR fetal growth retardation |
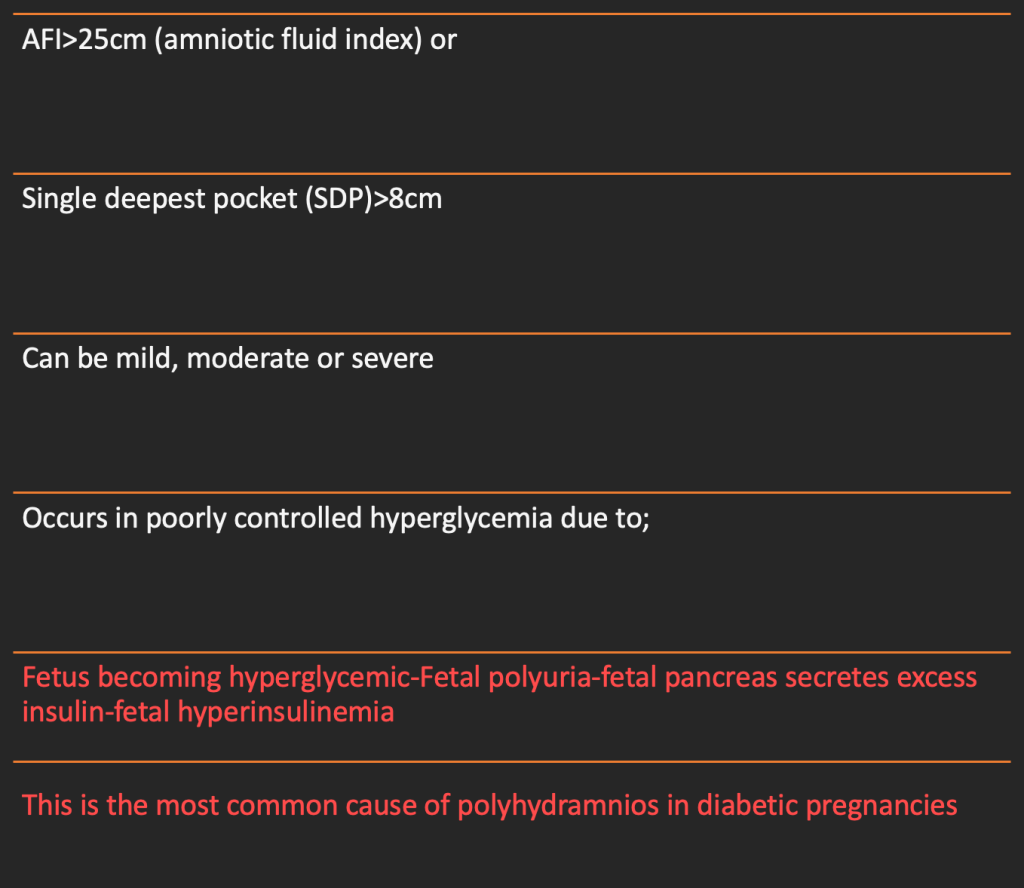
2. Poly Hydramnios
3. Infection
Why diabetic pregnancies have more infections?
A. impaired immunity
Hyperglycemia in pregnancy significantly increases maternal susceptibility to bacterial, fungal and urinary infections
B. Glucosuria- provides a growth medium for bacteria especially E Coli, increasing UTI risk.
C. Increased vaginal glucose-promotes recurrent candidiasis.
D. Poor glycemic control
E. Vascular changes:
Common Infections
| 1 – UTI including asymptomatic bacteruria, more cystitis, higher incidence of pyelonephritis |
| Common organisms: E. Coli, Klebsiella, Proteus, Group B Streptococcus |
| 2 – Vaginal candidiasis |
| 3 – Soft tissue infections: skin abscess, cellulitis, Fungal infections (intertrigo) |
| 4 – Post operative wound infections |
| 5 – Resiratory infections |
| 6 – Grp B streptococcus colonization –This increases neonatal sepsis, chorioamnionitis and preterm labor |
Other Maternal short-term outcomes
4. Increased operative delivery:
- Cesarean section
- Instrumental delivery due to macrosomia
5. Difficult labors (Shoulder dystocia Birth trauma)
6. Diabetic ketoacidosis (DKA) – more common in type 1 diabetes
7. Worsening of diabetic complications in pre-existing diabetes:
- Retinopathy progression
- Nephropathy worsening
8.Hypoglycemia episodes (if on insulin)
B. Long-term Maternal outcomes
- High risk of developing type 2 DM
- Higher risk of GDM in future pregnancies
- Increased Cardiovascular risk
- Long term metabolic syndrome
- Persistent microvascular complications in those with preexisting diabetes
Short term Fetal/Neonatal outcomes
- Macrosomia
- Fetal overgrowth of shoulders and trunk-risk of shoulder dystocia
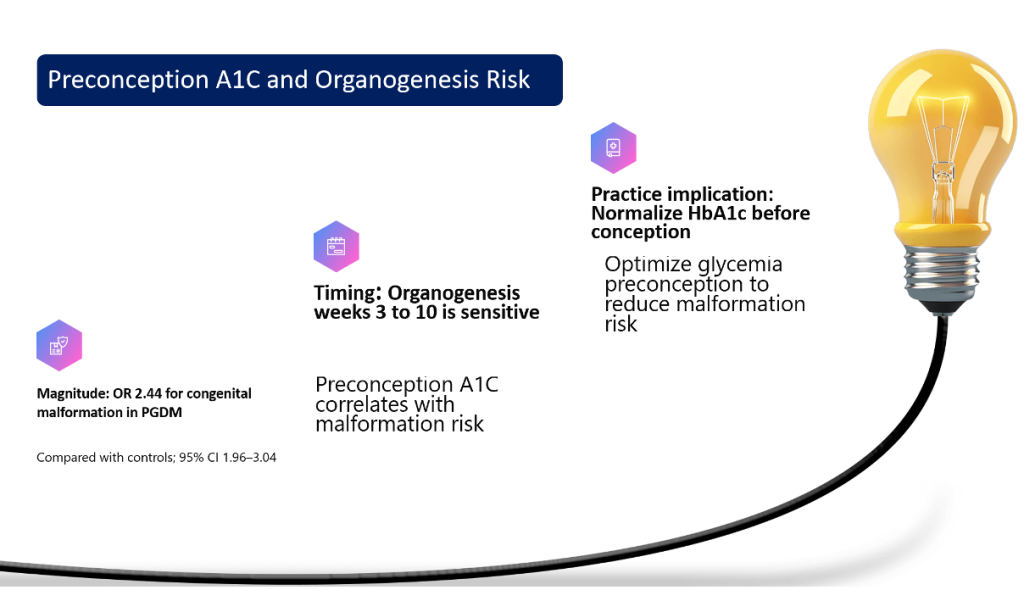
- Congenital anomalies:
- Neural tube defects
- Cardiac anomalies
- Caudal regression syndrome
Barker Hypothesis
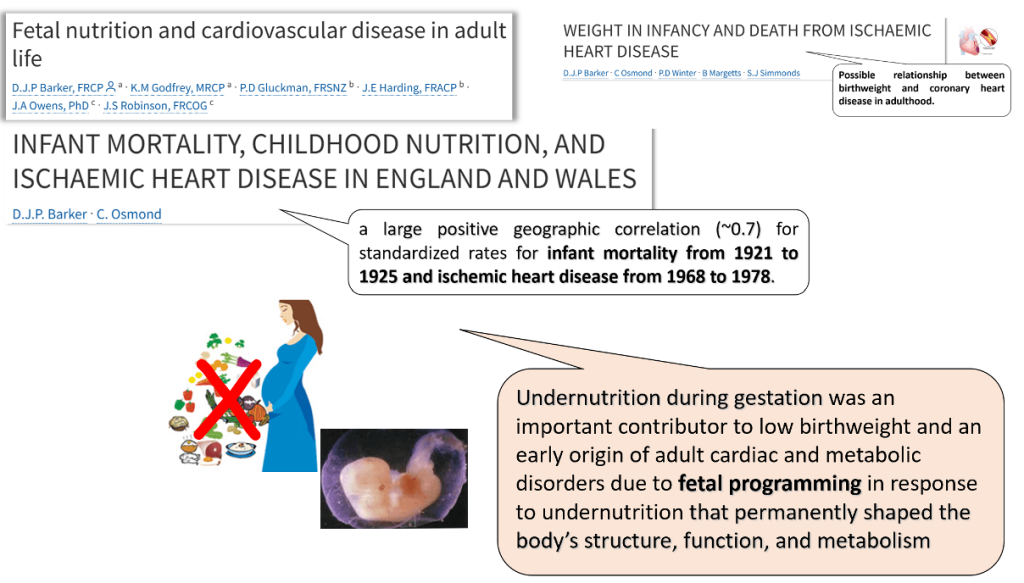
- “Two decades ago, a British physician named David Barker noticed an odd correlation on a map: the poorest regions of England and Wales were the ones with the highest rates of heart disease. Why would this be, he wondered, when heart disease was supposed to be a condition of affluence — of sedentary lifestyles and rich food?
- He decided to investigate, and after comparing the adult health of some 15,000 individuals with their birth weight, he discovered an unexpected link between small birth size (1921-25) — often an indication of poor prenatal nutrition — and heart disease in middle age (1968-78).
- Faced with an inadequate food supply, Barker conjectured, the fetus diverts nutrients to its most important organ, the brain, while skimping on other parts of its body — a debt that comes few decades later in the form of a weakened heart.”
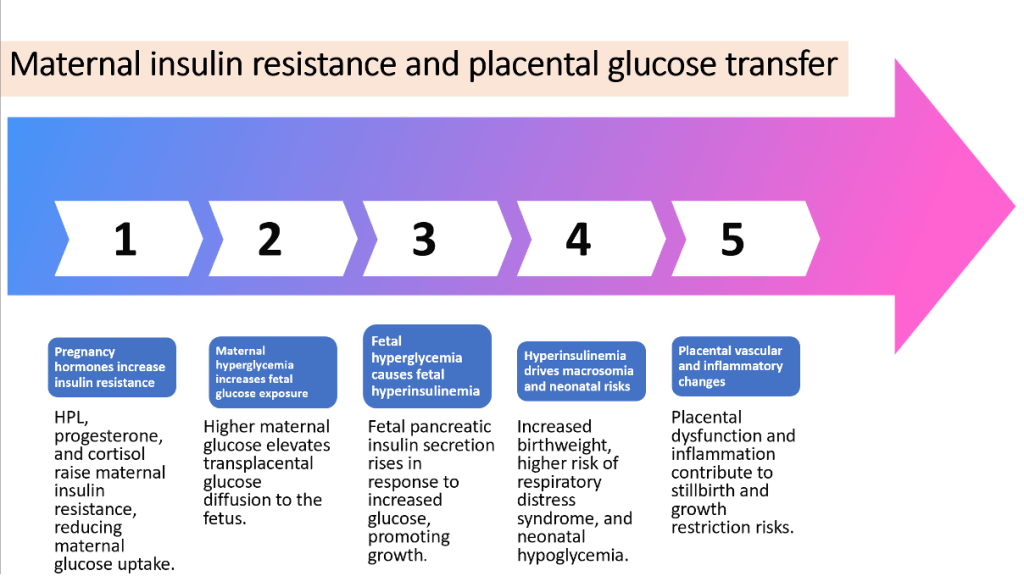
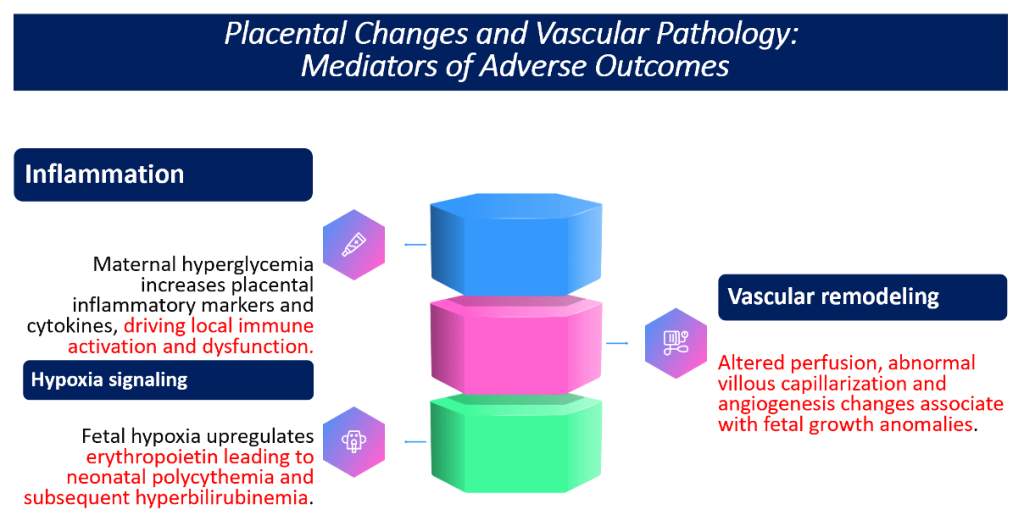
Placental Changes and Vascular Pathology: Mediators of Adverse Outcomes
Preconception A1C and Organogenesis Risk
Most Important Message
All women should be screened for Gestational Diabetes Mellitus, during the first visit, even if they have no symptoms. And treated for hyperglycemia optimally.
Short- and Long-term Impact of treatment
Impact of insulin therapy
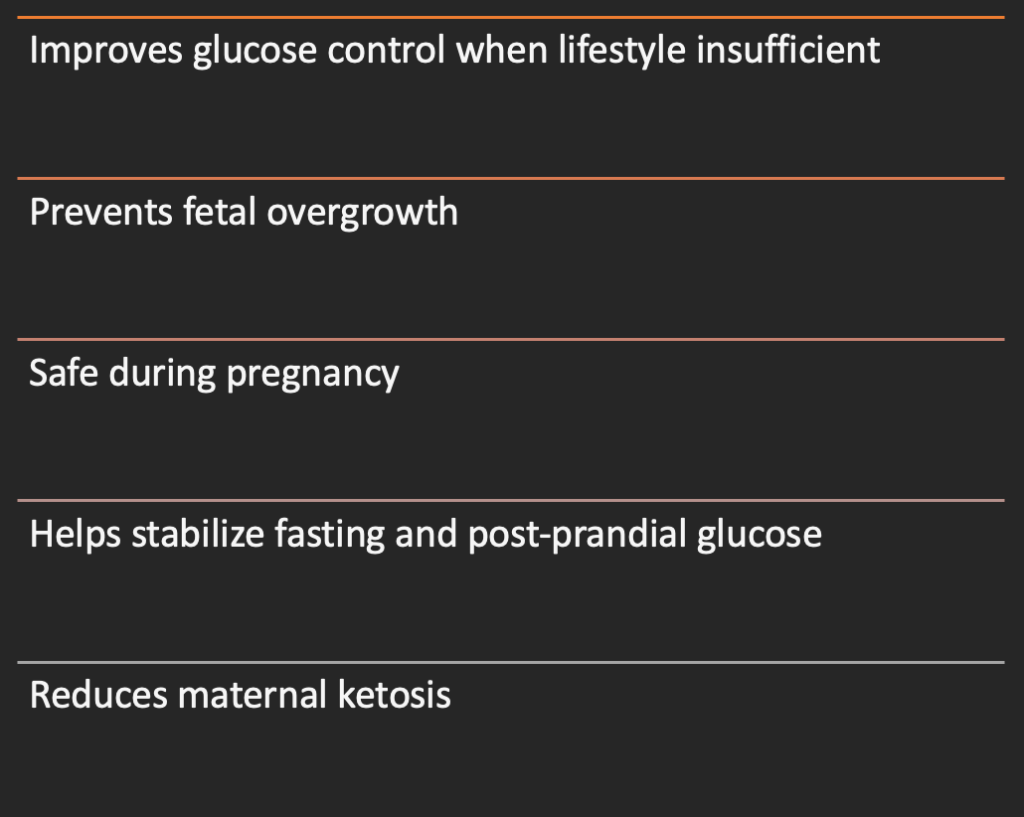
Impact of Metformin

Long-term impacts of treatment
| Effective treatment lowers risk of: |
| Progression to Type 2 diabetes |
| Future cardiovascular disease |
| Recurrent GDM in later pregnancies |
| Chronic hypertension |
| Metabolic syndrome |
| Long-term microvascular complications in type 1/2 diabetes |
Impact of future pregnancies
| Treatment reduces future: |
| Recurrent GDM (risk decreases by 20–40% |
| Macrosomia in subsequent pregnancies |
| Risk of preeclampsia in future pregnancies |
| Complications from uncontrolled diabetes |
Prevention of Intergenerational Diabetes
Implications for Practice
- Early screening (even before 24–28 weeks) for women at risk (e.g., obesity, family history, previous GDM) may help identify those with hyperglycemia sooner.
- Tight glucose control, appropriate lifestyle and nutritional management, and individualized pharmacotherapy can help reduce adverse outcomes.
- Enhanced postpartum follow-up is crucial, as up to 60% of women with GDM may not return for glucose monitoring, risking undiagnosed type 2 diabetes later.
Key Take-Aways
| Treatment of hyperglycemia has major immediate and long-term benefits |
| Protects both mother and baby from metabolic complications |
| Lifestyle therapy is first-line; insulin added when needed |
| Good glycemic control = improved pregnancy outcomes |
| Long-term follow-up improves maternal and child health, reduces the national and global burden |
References:
- Suvarna R, Shetty S. Effectiveness of continuous glucose monitoring on maternal and neonatal outcomes in gestational diabetes mellitus: a systematic review and meta-analysis. BMC Pregnancy and Childbirth. 2026; 30 Jan. doi:10.1186/s12884-026-08663-8 — this review shows links between glucose monitoring and improved pregnancy outcomes in GDM.
- American Diabetes Association Professional Practice Committee. Management of diabetes in pregnancy. Diabetes Care. 2026;49(Suppl 1):S321–S338 — ADA’s 2026 standards include updated evidence on maternal and neonatal risks of hyperglycemia and care recommendations.
- McLaren R, et al. A proposed classification of diabetes mellitus in pregnancy with implications for maternal and neonatal outcomes. American Journal of Obstetrics and Gynecology. 2026; (in press). doi:10.1016/j.ajog.2026.00061.X — outlines updated classification and outcome implications of dysglycemia in pregnancy.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs