

CME INDIA Presentation by Dr. Richa Manaswita,MBBS, DGO, DNB (Obstetrics & Gynecology), Consultant Gynecologist & Obstetrician, Department Head – Obstetrics & Gynecology, Soni Hospital, Jaipur.
Based on presentation at CID 2025,Mumbai.
Over a decade of clinical expertise in women’s health, high-risk pregnancies, and endocrine-related gynecological disorders.
- Special focus on diabetes in pregnancy, thyroid disorders, and drug safety in maternal care.
- Lead consultant for maternal–fetal care protocols and interdepartmental coordination at Soni Hospital.
- Active member of FOGSI, IMA, and Jaipur Gynae Society.
- Authored and presented research on drug safety, fetal outcomes, and management of comorbidities in pregnancy.
- Strong advocate for integrating evidence-based medicine with compassionate, patient-centered care.
What happens when glucose meets gestation?
- Globally about 1 in 6 births (~15–16%) are affected by GDM.
- Pre-gestational diabetes affects roughly 1% of pregnancies.
- (Type 2 ≈8%, Type 1 ≈2%).
- Poorly controlled maternal glucose is strongly teratogenic: —-first-trimester Hba1c >10% can yield up to a 25% risk of major congenital malformations.
- Diabetes in pregnancy increases risk of miscarriage, preterm birth, preeclampsia and neonatal complications (macrosomia, hypoglycemia).
- Optimal treatment improves outcomes, thus we emphasizing the importance of managing maternal glucose levels
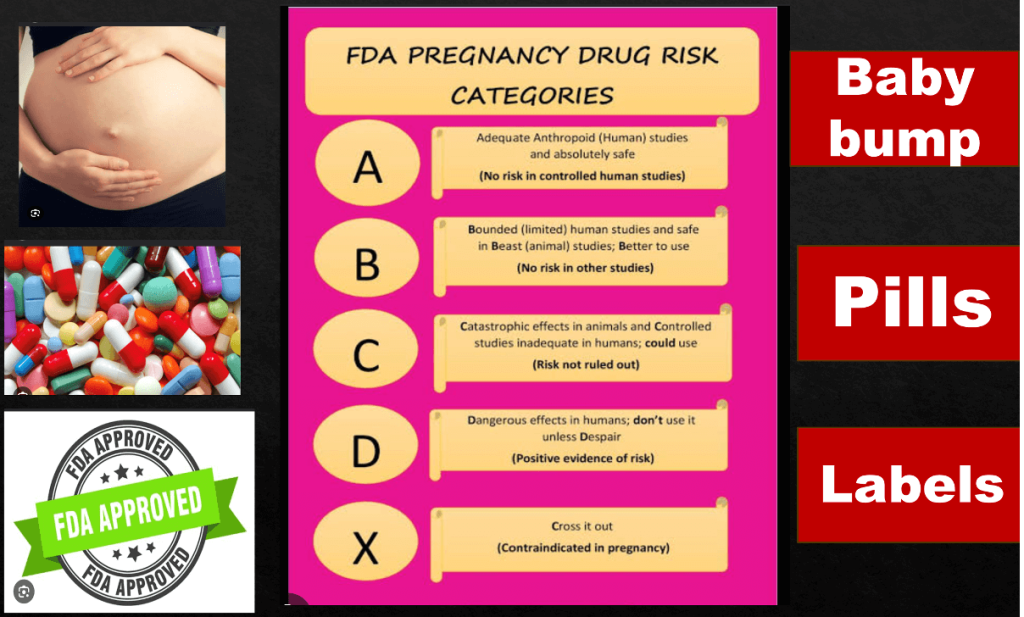
Prescribing For 2 = Medication Safety Matters in Pregnancy
- Only a small percentage of drugs are contraindicated for use in pregnancy or while breast feeding. -e.g., isotretinoin, mycophenolates.
- For the majority of drugs, labeling should provide what is known in a way that enables decisions for treatment.
The question is HOW?
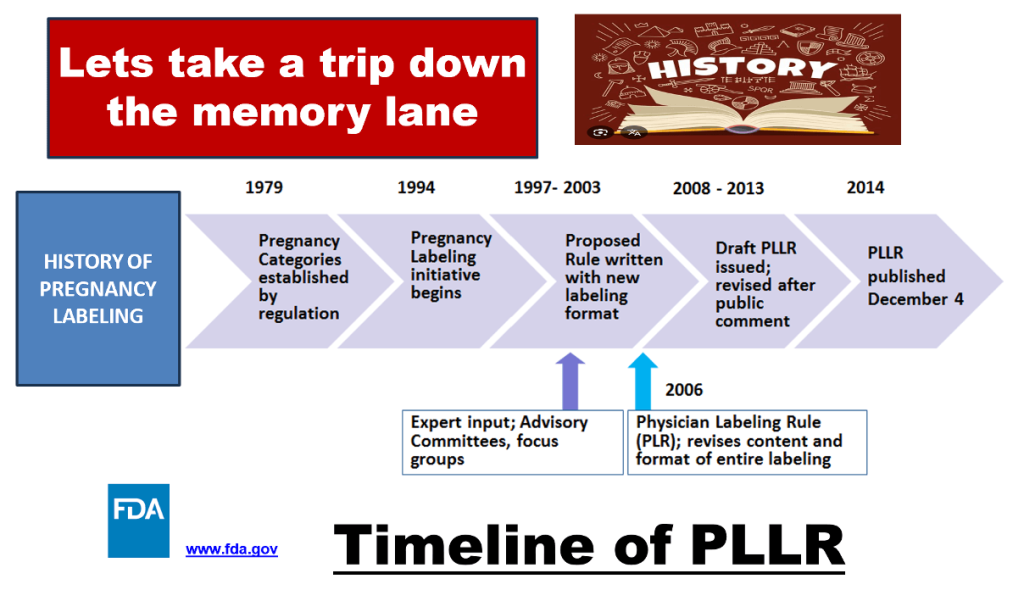
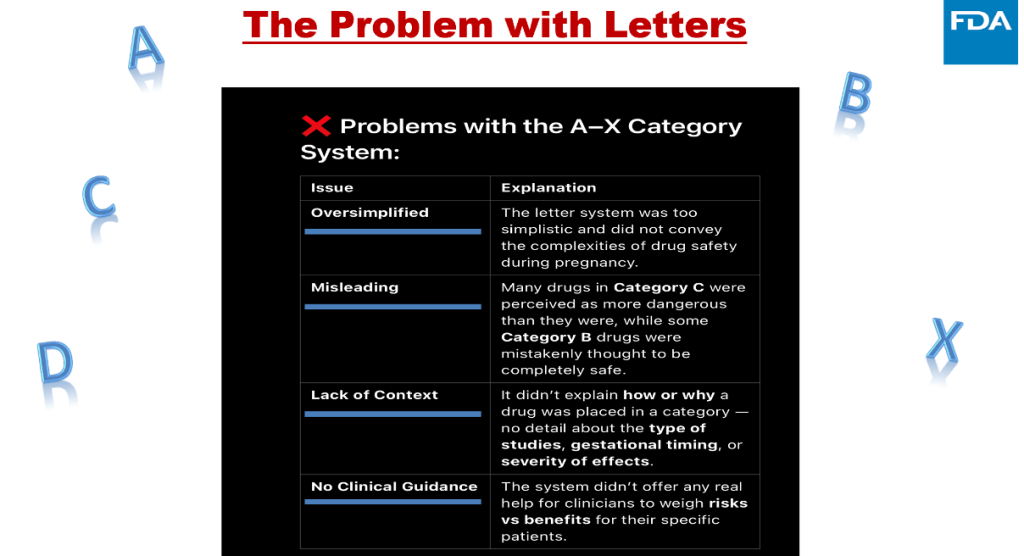
The Problem with Letters
Intent of PLLR
| Provide the prescriber with relevant information for critical decision-making when treating pregnant or lactating women |
| More complete statement of the known risks based on the available data |
| Considerations of medical/disease factors |
| Animal data put in context of human exposure |
| Human data added when available |
| Explicitly states when no data are available |
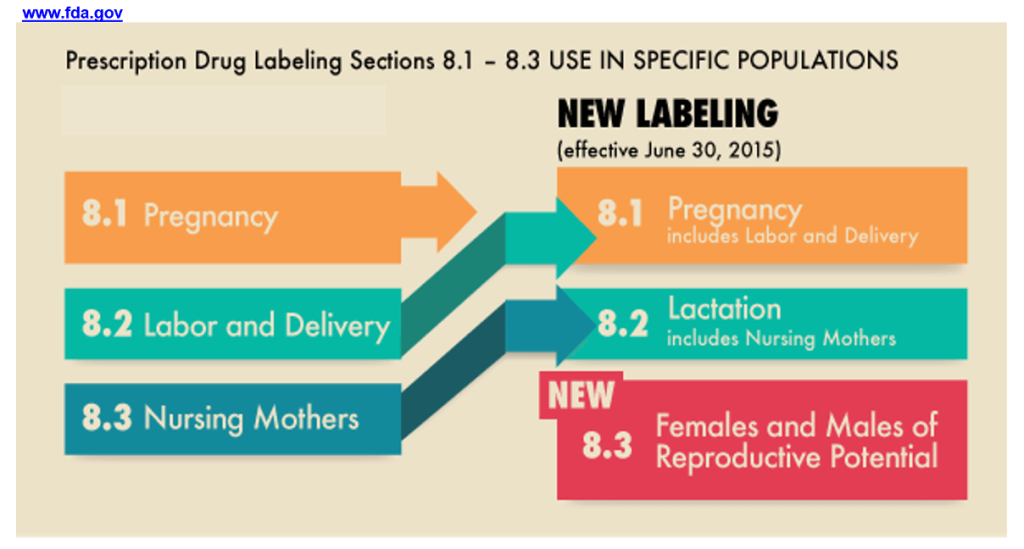
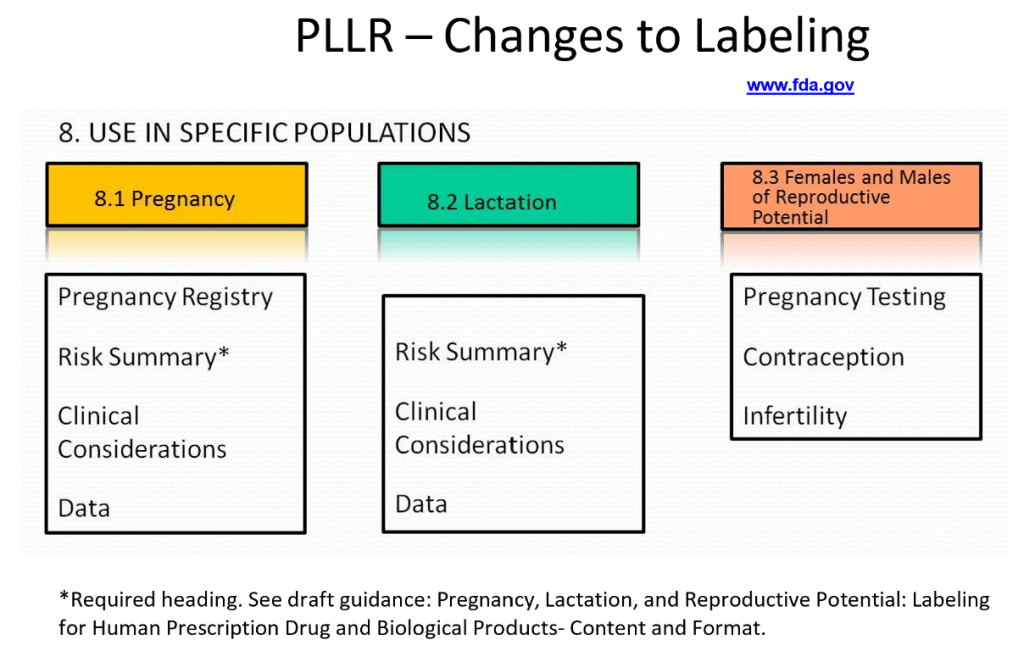
PLLR – Changes to Labeling
2 LIFES 1 PLAN – GUIDELINES DRIVEN DIABETES CARE
- NICE (UK): If GDM is uncontrolled by diet in 1–2 weeks, start metformin ; add insulin if targets still unmet .
- For fasting ≥7.0 mmol/L or macrosomia/hydramnios in usg , begin insulin ± metformin immediately .
- Rapid-acting analogues (aspart/lispro) are explicitly preferred over human insulin .
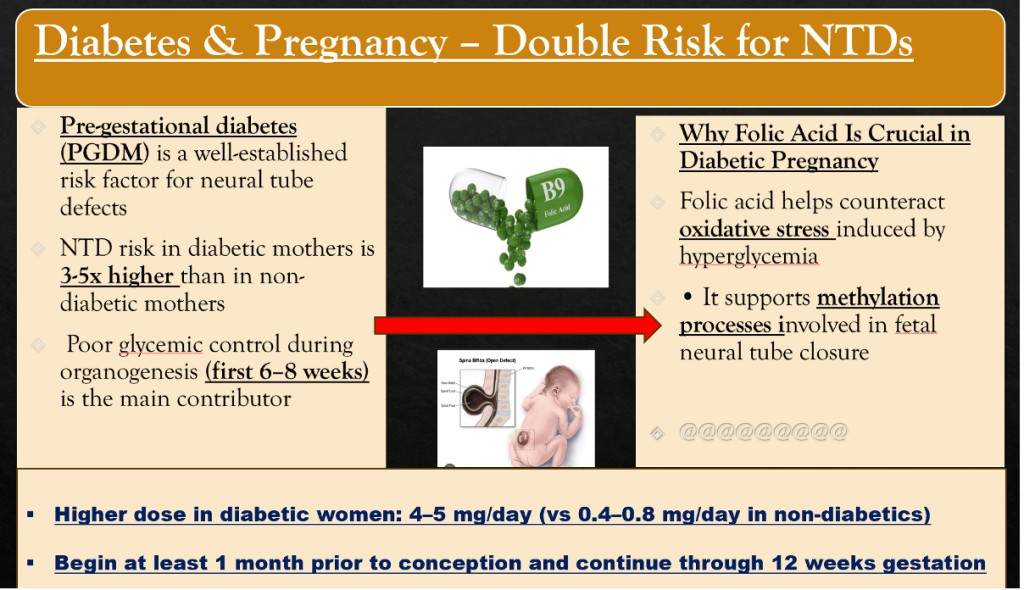
- For pregestational diabetes, NICE and ADA recommend preconception counseling, folate 5 mg, and switching off teratogenic drugs (statins, ACEi)
Shots vs swallows the Great GDM debate
- Insulin is the gold-standard therapy for both pregestational and gestational diabetes.
WHY?
| injected insulins do not cross the placenta, making them very safe. |
| Rapid-acting analogues (insulin aspart, lispro) have proven safety and better postprandialcontrol than human regular insulin. |
| They reduce hypoglycemia and improve glucose control, and are generally preferred over regular insulin. |
| Basal insulins: Intermediate (NPH) and long-acting analogues (detemir, glargine) may be used.Studies show detemir yields comparable or better outcomes than NPH. |
| ADA/ACOG endorse any insulin regimen that achieves glycemic targets; they specifically note lispro/aspart and detemir as well-studied. |
| In practice, multiple daily injections (basal+bolus) or insulin pump therapy are common. Continuous glucose monitoring (CGM) is recommended for type 1 pregnancy to improve control. |
Metformin (FDA Cat B):
| Crosses the placenta, but many trials show no increase in fetal malformations. |
| It can improve maternal weight gain and lower hypertension risk. |
| NICE and others allow metformin as first-line pharmacotherapy for GDM (if diet fails in 1–2 weeks). |
| Its downsides are maternal GI side effects (diarrhea, nausea) and the need for supplemental B12. |
Glyburide/Glibenclamide
| A sulfonylurea oral agent sometimes used in GDM (if metformin not tolerated). |
| It is the only sulfonylurea tested in large trials of pregnancy. |
| Efficacy is similar to insulin for glycemic control, but outcomes are less favorable: |
| Infants of glyburide-treated mothers tend to have higher birth weights and more neonatal hypoglycemia compared to insulin. |
| For example, one meta-analysis found >2× higher odds of neonatal hypoglycemia on glyburide vs insulin. |
| Thus, many experts prefer metformin or insulin over glyburide, except when injections are impossible. |
Infants of glyburide-treated mothers tend to have higher birth weights and more neonatal hypoglycemia compared to insulin.
Choosing wisely- a comparative lens on diabetic drugs
- Insulin vs Metformin (GDM):
| Recent meta-analyses find metformin matches or beats insulin for neonatal outcomes. |
| One analysis (5,964 patients) showed metformin vs insulin significantly lowered macrosomia (RR≈0.66), NICU admission, neonatal hypoglycemia (RR≈0.67) and LGA rates, with less maternal weight gain and fewer C-sections . |
| There were no differences in perinatal mortality or birth trauma. |
| In short, metformin-treated pregnancies had fewer large babies and neonatal complications than those treated with insulin. |
| Maternal glucose control was comparable, though some studies note slightly higher fasting glucose on metformin. |
Metformin vs Glyburide:
- A Cochrane review found no significant difference between metformin and glyburide for most key outcomes (preeclampsia, cesarean, large babies, neonatal hypoglycemia) .
- However, one trial noted fewer composite adverse outcomes with metformin
- In general, metformin and glyburide control glucose similarly, but metformin tends to be favored because it causes less weight gain and appears safer for the baby (no increased neonatal hypoglycemia in large trials).
- Glyburide performs worse. Compared to insulin, glyburide led to higher birth weights and a 50% increased risk of neonatal hypoglycemia.
- Another study noted more macrosomia and neonatal hypoglycemia with glyburide than with insulin. Thus, insulin remains superior.
- These data have led many centers to prefer metformin over glyburide as the primary oral agent in GDM. An international review concluded “metformin can decrease the incidence of perinatal complications” and is a generally safe alternative to insulin
Immunize Without Compromise
Are TT (Tetanus Toxoid/Tdap) and Influenza Vaccines Safe in Pregnant Diabetic Patients?
Should We Give TT and Flu Vaccines to Pregnant Diabetics?
What are the Benefits?
| The answer to the first question is resounding yes |
| Influenza: ~40–60% efficacy in general adults; protects diabetic mother and fetus from severe flu, pneumonia, and poor glycemic control. |
| TT/Tdap: Protects neonate from pertussis with no fetal or maternal harm. |
| For diabetics, flu vaccine reduces severe complications and mortality significantly. |
What Are The Measures to Ensure Safe Vaccination in Pregnant Diabetics?
- Pre-vaccination glycemic check Ensure blood glucose is within target range.
- Timing TT/Tdap: best at 27–36 weeks; can be administered anytime for need.
- Flu vaccine: anytime during flu season, any trimester.
- Can administer TT and flu concurrently at different injection sites.
- Remember to give Inactivated formulations.
- Monitor post-vaccination Check sugars 24–48 hrs post-vaccine to detect any transient rise.
- Patient counseling Educate on benefits vs. minor risks; address hesitancy.
The Burning Dilemma- Safe Uti Care In Pregnancy
- Prevalence: UTIs affect 8% of pregnant women; gestational diabetes mellitus (GDM) increases UTI risk by ~20% (pooled OR 1.2, 95% CI 1.1–1.3).
- Additional diabetes risk: Diabetic individuals have a 1.6-fold higher risk of genitourinary infections.
- UTI itself worsens glycemic control due to infection-induced stress hyperglycemia.
UTI – Drug Pregnancy Safety Glycemic Impact
| Nitrofurantoin—-OK 2nd trimester; slight fetal risk if near term No known effect Safe if renal fxn normal Avoid near term (<38 wks). |
| Fosfomycin Safe throughout No impact Safe Single-dose therapy. |
| Amoxicillin/Clavulanate Safe (Penicillin class) No impact Safe Confirm sensitivity due to resistance. |
| 1st/2nd Gen Cephalosporins Safe (e.g., cephalexin) No impact Safe Preferred broad coverage. |
| TMP-SMX Avoid in 1st trimester and near term No data Use only if necessary Risk of neural tube defects & neonatal jaundice. |
| Fluoroquinolones Contraindicated: fetal cartilage toxicity n/a Avoid Reserved for multidrug-resistant cases. |
Does Folic Acid Affect Glycemic Control?
Recent Innovations:
| Combined formulations: Folic acid + myo-inositol + B12 for diabetic & obese pregnant women. |
| Epigenetic insight: Folate plays a role in DNA methylation affecting fetal programming. |
| Pharmacogenetics: Tailoring folic acid dose based on MTHFR polymorphisms. |
| Folic acid nanoformulations: Under development for better placental transport. |
| Inositol (Myo-inositol) Improves insulin sensitivity May reduce GDM and NTD risk – emerging evidence. |
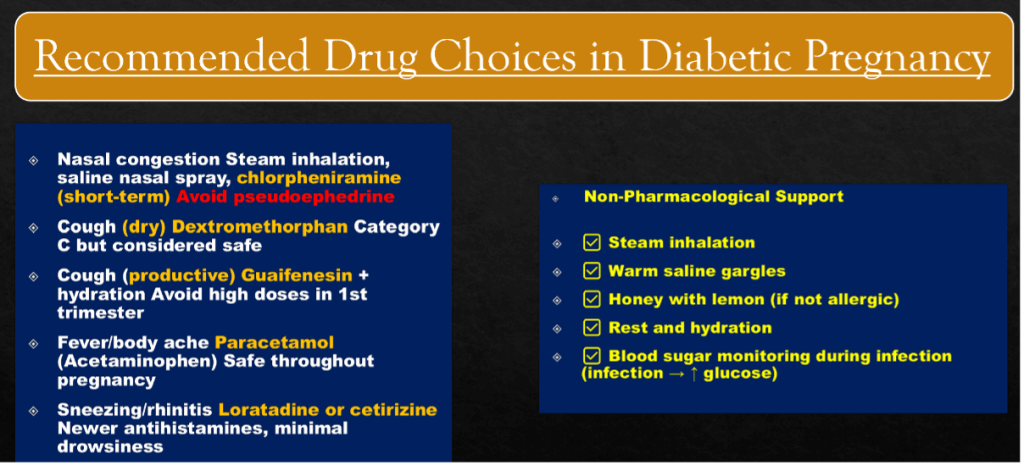
Don’t Let the Common Cold Tip the Sugar Scale in Pregnancy
- Pregnancy + Diabetes (GDM or Pre-GDM) = High-risk for both mother and fetus
- Infections (like URTI) are common, but treatment is challenging due to:
- Teratogenic risk
- Potential glycemic disturbances
- Placental transfer
- Immune modulation
Which cough syp spoon, are safe in pregnancy
| Antihistamines Chlorpheniramine, Diphenhydramine, Loratadine Yes (Category B) Neutral. |
| Decongestants Pseudoephedrine, Phenylephrine Avoid in 1st trimester, monitor BP Can ↑ glucose. |
| Antitussives Dextromethorphan Yes (Cat C), no teratogenicity Neutral. |
| Expectorants Guaifenesin Caution in 1st trimester Minimal impact. |
| Antipyretics Paracetamol Yes (safe in all trimesters) No effect. |
| Lozenges Menthol, Honey-based Yes No effect. |
| Antibiotics (if infection suspected) Amoxicillin, Azithromycin Yes Neutral. |
| Pseudoephedrine Decongestant May ↑ insulin resistance Use with caution, avoid in 1st trimester. |
| Phenylephrine Decongestant Vasoconstrictive – may increase BP & glucose Avoid in pregnancy. |
| Oral steroids (if used) Anti-inflammatory Significant ↑ glucose Avoid unless severe inflammation. |
| NSAIDs (e.g., Ibuprofen) Analgesic Potential for ↑ glucose Avoid in 3rd trimester. |
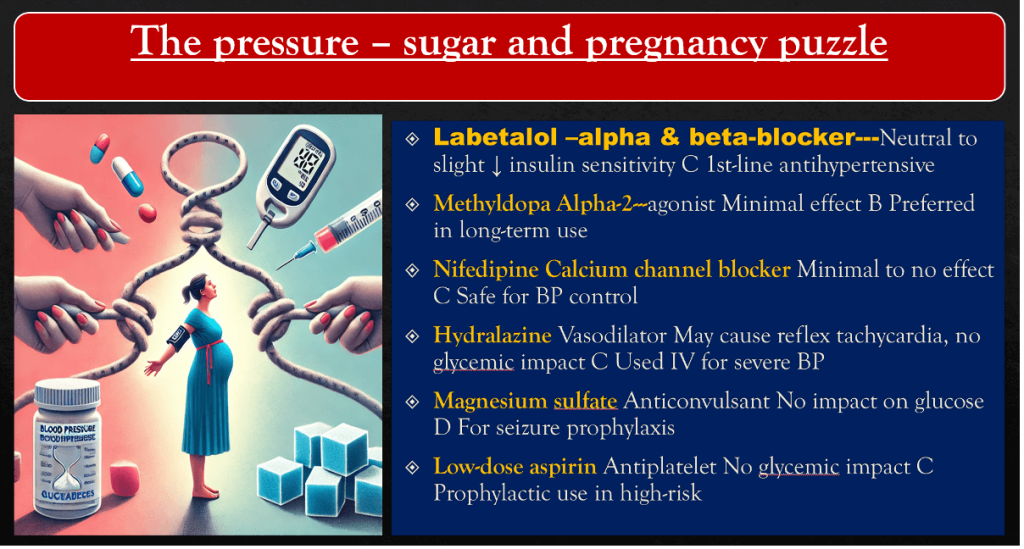
Pressure, sugar and pills: walking the tightrope in pregnancy
- Managing preeclampsia in a patient with gestational or pregestational diabetes is complex because:
- Both conditions involve vascular dysfunction and oxidative stress.
- Many drugs used for preeclampsia can alter glucose metabolism.
- Glycemic control is crucial for both maternal and fetal outcome.
The pressure – sugar and pregnancy puzzle
Advances in Preeclampsia Management:
- sFlt-1/PlGF Ratio Testing Early detection of preeclampsia.
- Pravastatin (under research) Prevents endothelial dysfunction.
- Metformin Used in obese/diabetic patients.
- Low-dose Sildenafil (experimental) Enhances uteroplacental perfusion.
- Customized insulin protocols during steroid therapy Reduces post-steroid hyperglycemia.
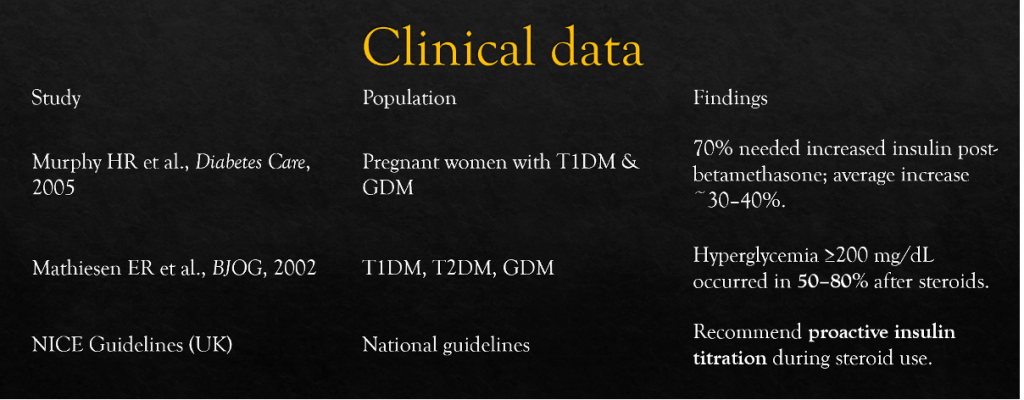
Breath For The Baby, Sugar Burden For The Mother – Steroids!
- Mechanism: Steroids increase insulin resistance and promote hepatic gluconeogenesis.
- Impact: Can lead to acute hyperglycemia (within 6–12 hours post-administration).
- Peak insulin resistance typically occurs 24–48 hours post-dose.
- May require doubling or tripling of insulin doses temporarily.
Implications & Alternates
- Clinical Implications:
- Monitor glucose every 2–4 hours for at least 72 hours.
- May require IV insulin infusion in inpatient settings.
- Risk of DKA is increased, especially in Type 1 diabetics.
Are There Alternatives?
- No current clinical equivalent to corticosteroids for fetal lung maturity.
- However, research is exploring:
- Minimal-dose regimens to reduce hyperglycemia.
- Delayed single-dose strategies (ongoing trials, e.g., ANZICS).
- Inhaled corticosteroids: Studied but not as effective systemically for fetal benefit.
Harmonal Harmony- Thyroid Disorders
- Thyroid disorders in pregnancy demand careful management to avoid fetal complications and glycemic disturbances.
- Most common: Hypothyroidism (2–3%) and Hyperthyroidism (0.2–0.4%)
- Goal: Maintain euthyroidism and stable glucose levels.
Prevalence & Significance
- Hypothyroidism: 2–3% of pregnant women
- Hyperthyroidism: 0.2–0.4% of pregnancies
- Implications:
- Miscarriage
- Preeclampsia
- Neurodevelopmental issues
- Glycemic instability
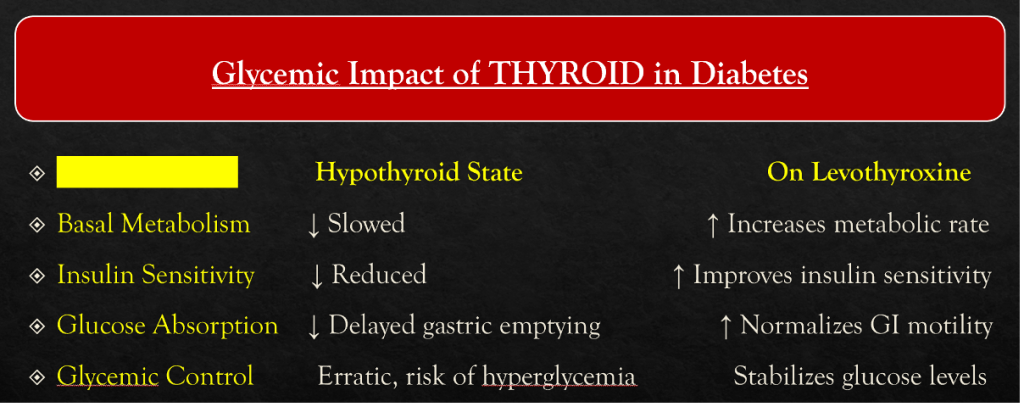
Hypothyroidism – Drug Choices
- Levothyroxine – Drug of choice——–Mechanism of Action:
- Synthetic T4 hormone → converted to active T3 peripherally → regulates metabolism and insulin sensitivity.
- Initial dose: ~1.6 mcg/kg/day, Dose may increase by 30–50% in early pregnancy due to increased TBG and placental metabolism.
- Monitoring:———-TSH every 4–6 weeks.
- Target TSH:
- 1st trimester: 0.1–2.5 mIU/L
- 2nd trimester: 0.2–3.0 mIU/L
- 3rd trimester: 0.3–3.0 mIU/L
Hyperthyroidism – Drug Choices
- 1st trimester: PTU (lower teratogenicity)
- 2nd–3rd trimester: Switch to Methimazole
- Beta-blockers (e.g., propranolol): Short-term use only
- Avoid overtreatment to prevent fetal hypothyroidism.
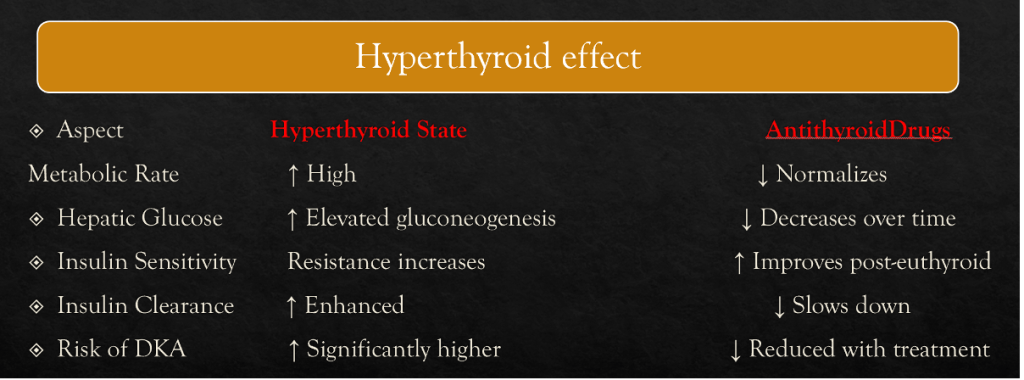
Comparative Glycemic Impact
- Levothyroxine: ↑ insulin needs as euthyroidism restored
- PTU: Mild hypoglycemia
- Methimazole: Mild insulin resistance
- Beta-blockers: Mask hypoglycemia symptoms
Recent Advances
- Levothyroxine dosing via body-weight algorithms
- FT4 monitoring apps
- Safer trimester-specific switching PTU/MMI
- Emerging thyrostatics under investigation
Antiepileptics in Pregnancy with Diabetes
- General → Use monotherapy, lowest effective dose; uncontrolled seizures are more dangerous than drug exposure.
- Avoid → Valproate (↑ neural tube defects, weight gain, insulin resistance, worsens glycemic control).
- Caution → Phenytoin & Phenobarbital (teratogenic, may worsen vitamin D & bone health in diabetic mothers).
- Safer choices →
- Lamotrigine (favorable metabolic profile, safer in pregnancy).
- Levetiracetam (minimal teratogenic risk, metabolically neutral).
- Carbamazepine – Acceptable but risk of spina bifida; monitor glucose closely.
- Folic acid → 4–5 mg/day pre-conception + pregnancy (especially crucial in diabetes).
- Vitamin K → Last month if on enzyme-inducing AEDs.
- Glucose monitoring → Pregnancy + AEDs + diabetes = ↑ risk of malformations; maintain tight glycemic control (HbA1c <6.5%).
- Breastfeeding → Allowed; monitor baby for sedation and mother’s sugar fluctuations.
Key line: In pregnant women with diabetes, avoid valproate, prefer lamotrigine/levetiracetam, give high-dose folate, control sugars tightly, and add Vit K if on enzyme-inducing AEDs.
References:
- https://www.acog.org/clinical#
- https://www.fda.gov/drugs
- https://www.rcog.org.uk/guidance/browse-all-guidance/scientific-impact-papers/diagnosis-and-treatment-of-gestational-diabetes-scientific-impact-paper-no-23/
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Superb…. very informative….useful in daily practice
Excellent