
CME INDIA Case Presentation by Dr. Viswesvaran, MD, DM, Senior Consultant- Interventional Pulmonology, Yashoda Hospitals, Somajiguda, Hyderabad.
CME INDIA Case Study
How Presented?
- 40-year male, non-smoker.
- Complaints of recurrent haemoptysis for 15 days.
- Supportive treatment given elsewhere and referred for evaluation and management.
Main Investigations
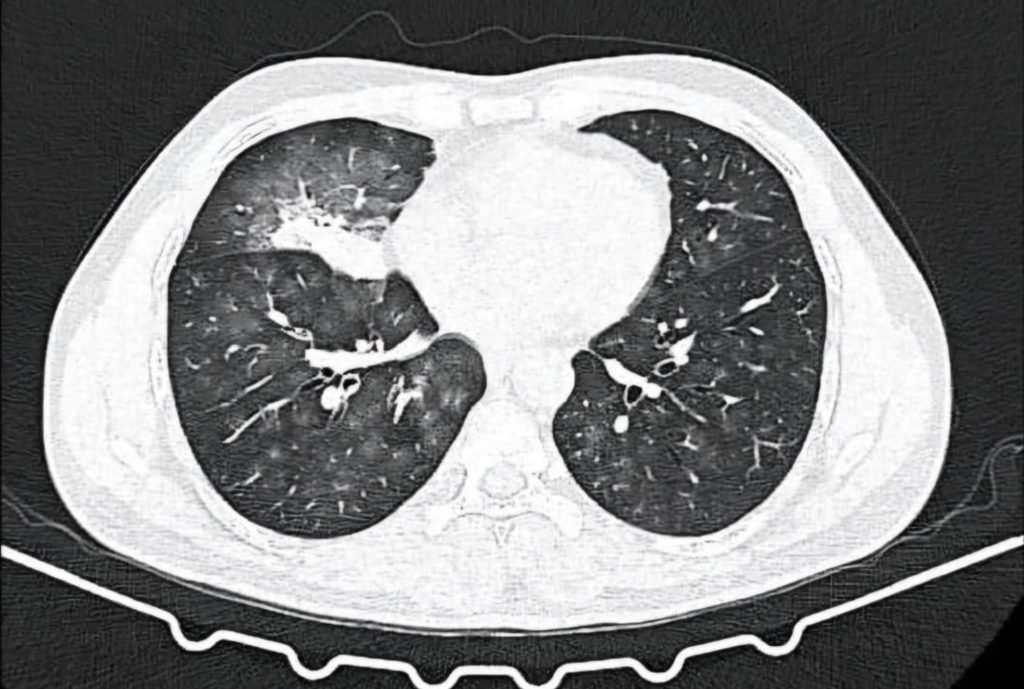
CT Thoracic angiography:
- Collapse consolidation of right middle lobe with ground glass opacities in bilateral lung fields.
- Hypertrophied bronchial collateral supplying area of consolidation.
- Bronchial artery embolization of feeder vessel done.
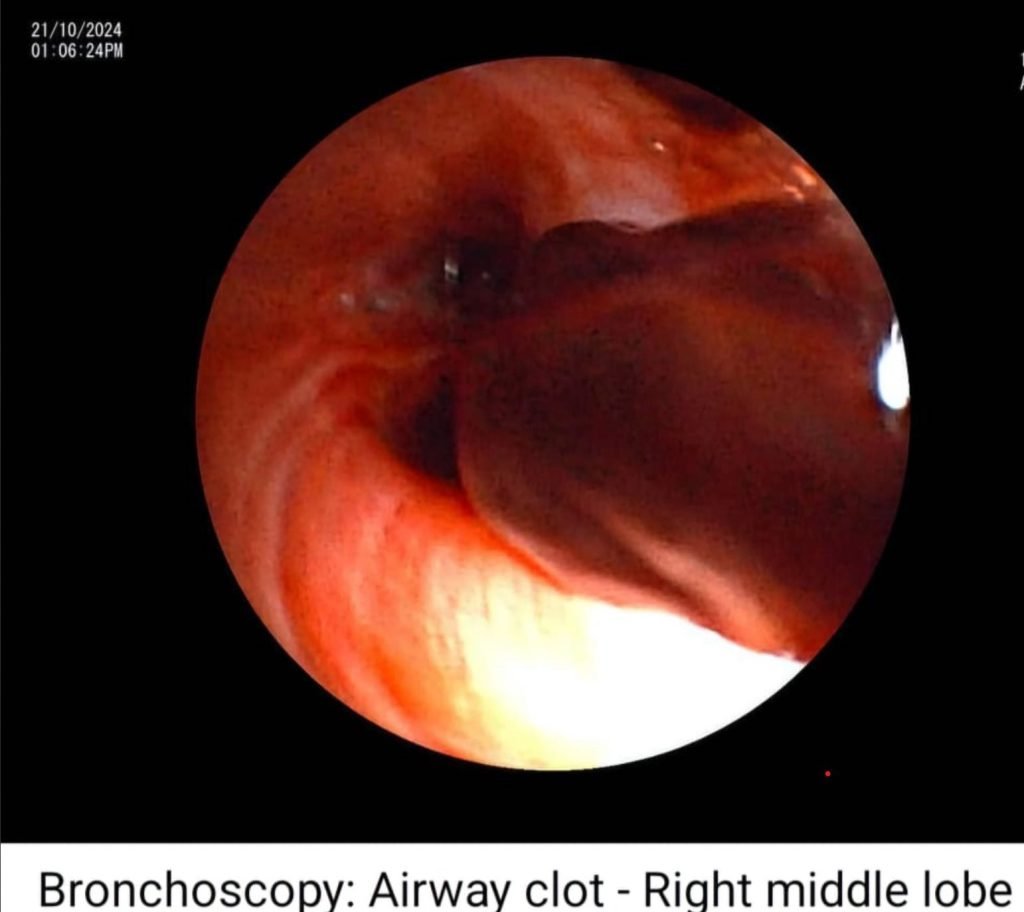
Bronchoscopy:
- Fresh bleed observed in trachea and right bronchial tree.
- Clot observed at the opening of right middle lobe bronchus.
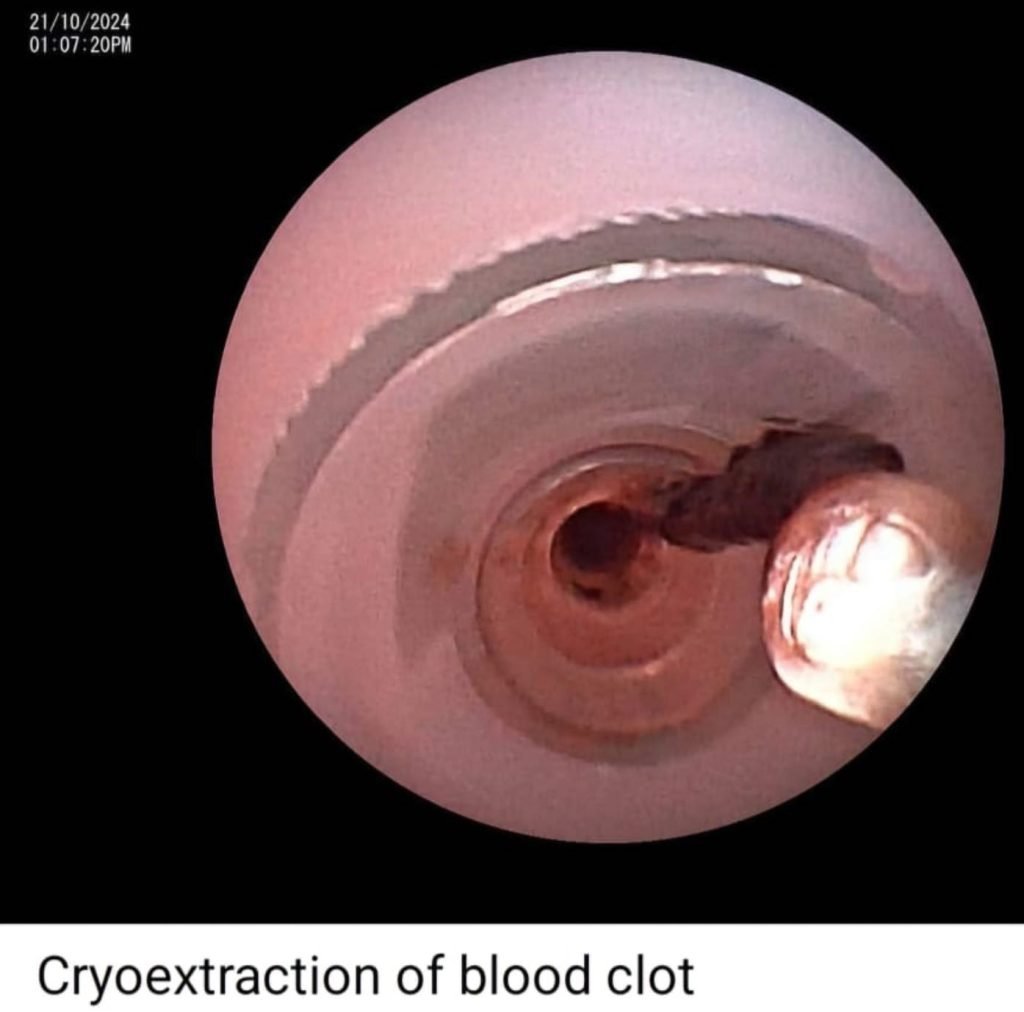
How Managed?
- Cryoextraction of blood clot done.
- Post clot removal – continuous airway bleed – could not be controlled with fogarty Balloon tamponade, local instillation of tranexamic acid and adrenaline.
- Rigid bronchoscopic intubation done.
- Watanabe sphigot 7 mm occlusion of right middle lobe bronchus done with glue instillation.
- Haemostasis achieved and extubated on table and shifted to ICU.


Ant synthetase antibody
- Positive
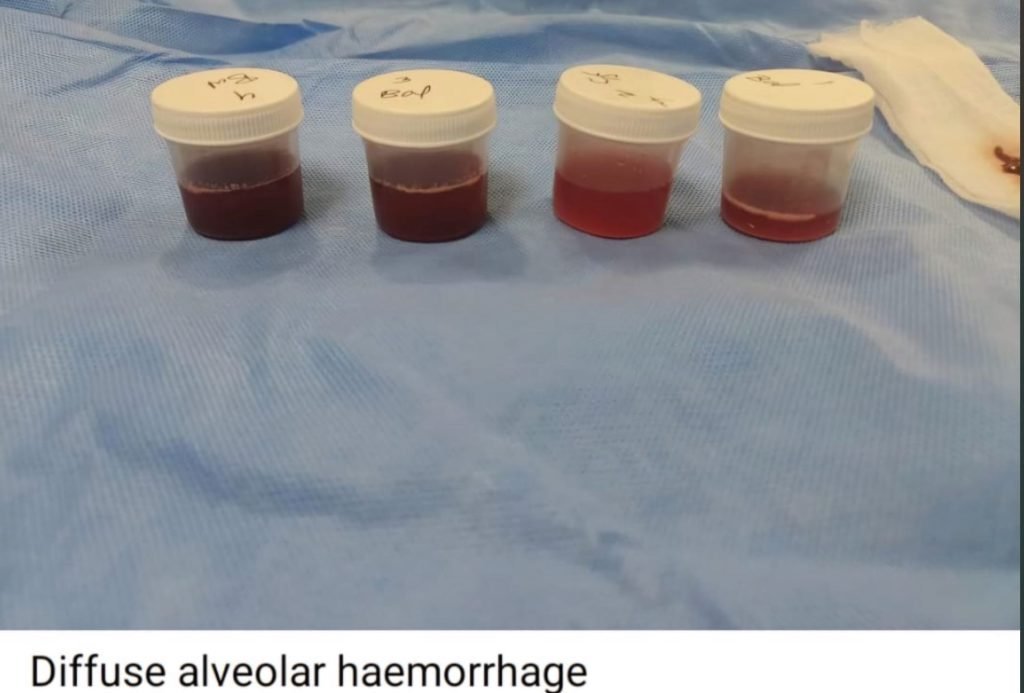
Diagnosis:
- Autoimmune DAH (Diffuse alveolar haemorrhage) secondary to ant synthetase antibody syndrome.
How Managed?
- Pulsed with steroids and cyclophosphamide.
- No recurrent haemoptysis with complete resolution of lung infiltrates. Patient discharged in stable state.
- Plan: Removal of sphigot after 2 weeks if no recurrence of bleed.
Learning points
1. Diffuse alveolar haemorrhage in ant synthetase antibody syndrome is rare. Can occur as the initial manifestation without other symptoms.
Pathogenesis: Pulmonary capillarity’s, Bland haemorrhage and Diffuse alveolar damage
2. Airway Sphigots (Watanabe) – Conical silicone plugs with studs (Available as – 7mm, 6mm, 5 mm)
Glue fixation of sphigot is done with cyanoacrylate- To avoid displacement of sphigot
CME INDIA Take Home Message
- Ant synthetase syndrome is a rare, chronic, immune-mediated disorder characterized by inflammation due to abnormal immune function and the presence of specific autoantibodies.
- It can affect multiple body systems and presents with a range of symptoms that vary in severity among individuals. Common symptoms include muscle inflammation (myositis), joint inflammation (polyarthritis), interstitial lung disease, and “mechanic’s hands,” marked by skin thickening, cracking, and discoloration of the fingers.
- Some individuals may experience Raynaud phenomenon, where fingers or toes turn white or blue and feel painful or numb in response to cold. Additional nonspecific symptoms can include fatigue, unexplained fevers, and unintended weight loss.
- While the exact cause is not fully understood, both genetic and environmental factors are believed to play a role. Ant synthetase syndrome can also co-occur with other rare inflammatory muscle diseases, such as dermatomyositis or polymyositis.
- Diagnosis: The diagnosis of ASS relies on clinical presentation alongside supportive investigations. Key diagnostic tools include:
Special Investigations
| – Elevated muscle enzymes (e.g., creatine kinase, aldolase) |
| – Detection of ant synthetase antibodies (ASAb) |
| – Electromyography (EMG) |
| – MRI of affected muscles |
| – Muscle biopsy |
| – Lung function tests and high-resolution CT scans of the lungs |
Diagnostic Criteria
| Presence of one or more ASAb targeting tRNA synthetase enzymes. |
| One or more of the following clinical features: interstitial lung disease (ILD), inflammatory myopathy, or inflammatory polyarthritis affecting small joints. |
| Patients with ILD should be evaluated for possible ASS. In cases mimicking rheumatoid arthritis (e.g., negative cyclic citrullinated peptide antibodies and nonerosive arthritis), ASS should be considered due to potential overlap. A “probable” diagnosis can be made if ILD and/or myopathy is present with ASAb. |
| Overlap Syndromes |
| Approximately 5-8% of ASS cases occur alongside other connective tissue diseases such as systemic lupus erythematosus, systemic sclerosis (SSc), or Sjögren’s syndrome. |
Details of the ant synthetase antibody test which was positive in this case
- It is a blood test used to detect the presence of specific autoantibodies associated with ant synthetase syndrome, an autoimmune condition. These autoantibodies target aminoacyl-tRNA synthetases, which are enzymes involved in protein synthesis. The most commonly identified antibody in this test is anti-Jo-1, but other ant synthetase antibodies such as anti-PL-7, anti-PL-12, anti-OJ, and anti-EJ can also be detected.
- The test helps in diagnosing ant synthetase syndrome and related autoimmune disorders. It is particularly useful in patients presenting with symptoms like myositis, interstitial lung disease, arthritis, and Raynaud phenomenon.
- Indications: This test is often indicated when there is clinical suspicion of ant synthetase syndrome, especially when a patient shows signs of unexplained muscle inflammation, lung involvement, or other systemic manifestations consistent with autoimmune diseases.
- Interpretation: A positive result supports the diagnosis of ant synthetase syndrome or a related autoimmune condition. The specific type of antibody detected may also provide information on the disease course, severity, and associated organ involvement.
- Clinical Relevance: Identifying these antibodies can guide treatment decisions and provide prognostic information, as different ant synthetase antibodies are associated with varying clinical outcomes and complications.
Case insights:
- Diffuse alveolar haemorrhage (DAH) in ant synthetase syndrome is a rare occurrence that can present as an initial manifestation without other systemic symptoms. The underlying pathogenesis involves pulmonary capillaritis, bland haemorrhage, and diffuse alveolar damage.
- Watanabe airway sphigots are conical silicone plugs with studs, available in 7mm, 6mm, and 5mm sizes. To prevent displacement, glue fixation of the sphigots is performed using cyanoacrylate.
CME INDIA Tail-Piece
- Video Link:
- The most common antibody associated with antisynthetase syndrome (ASS) is anti-Jo-1, named after John P., a patient with polymyositis (PM) and interstitial lung disease (ILD) first identified in 1980. This antibody is particularly prevalent in patients with pulmonary symptoms of ASS and is known to target histidyl-transfer RNA synthetase. Anti-Jo-1 antibodies are detected in approximately 68-87% of cases. Given that around 25% of patients with polymyositis or dermatomyositis (PM/DM) have antisynthetase antibodies, the estimated prevalence of ASAb is at least 3-4 per 100,000, considering that PM/DM has a prevalence of approximately 15 per 100,000.
References:
- Witt LJ, Curran JJ, Strek ME. The Diagnosis and Treatment of Antisynthetase Syndrome. Clin Pulm Med. 2016 Sep;23(5):218-226. doi: 10.1097/CPM.0000000000000171. PMID: 27594777; PMCID: PMC5006392.
- Cojocaru M, Cojocaru IM, Chicos B. New Insights into Antisynthetase Syndrome. Maedica (Bucur). 2016 Jun;11(2):130-135. PMID: 28461832; PMCID: PMC5394574.
- Targoff, Ira N. “Autoantibodies and their significance in myositis.” Current Rheumatology Reports 10.4 (2008): 333-340.
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs