

CME INDIA Case Presentation by Dr. Vinay Dhandhania, Diabetologist, Ranchi.
CME INDIA Case Study

How Presented?
- A 58-year-old male with a 12-year history of type 2 diabetes mellitus presented with frequent hypoglycaemic episodes interspersed with post-prandial hyperglycaemia despite apparently stable insulin dosing. He was receiving premixed human insulin twice daily.
- On directed history, the patient admitted to injecting exclusively in the periumbilical region and reusing the same syringe for 3–4 days. His medical history was significant for surgical management of renal cell carcinoma at a tertiary centre in Chennai.
Physical Examination
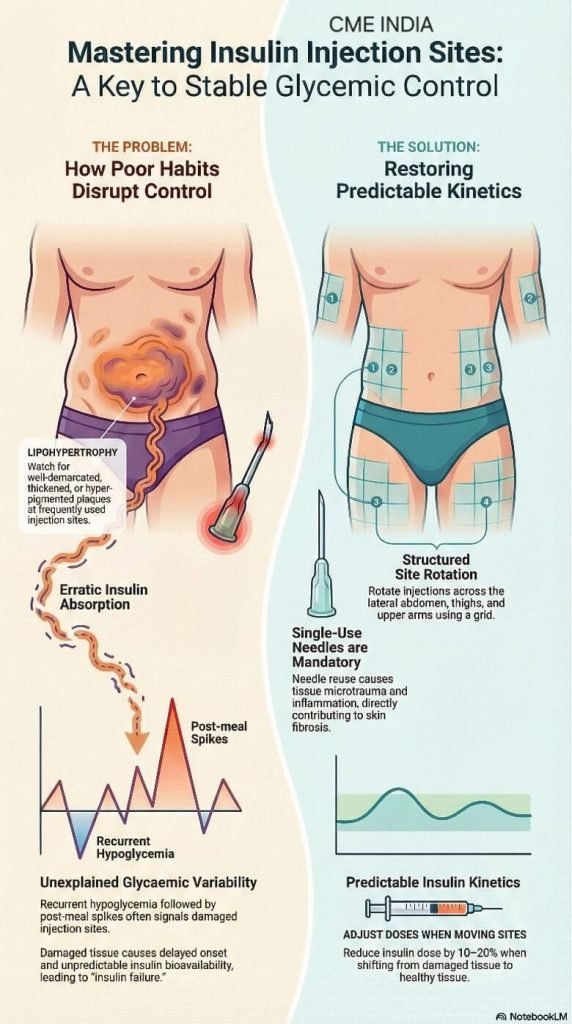
- Inspection of the abdomen revealed a large, well-demarcated, circular, darkly hyperpigmented plaque surrounding the umbilicus, with a central area of textural change and induration.
- The lesion was non-tender, without warmth or erythema. Palpation demonstrated altered subcutaneous consistency compared with surrounding skin.
- These findings were clinically diagnostic of advanced periumbilical lipohypertrophy with post-inflammatory hyperpigmentation and possible central lipoatrophy due to chronic microtrauma.
Glycaemic Pattern
- Self-monitoring records demonstrated marked day-to-day and within-day variability, including unexplained hypoglycaemic episodes and post-prandial spikes, consistent with impaired and unpredictable insulin absorption from lipohypertrophic tissue.
Pathophysiological Considerations
- Repeated insulin exposure at the same site promotes local anabolic effects on adipocytes, leading to hypertrophy, fibrosis, and altered microcirculation.Needle reuse further exacerbates tissue trauma through blunt needle tips, micro-tears, local inflammation, and increased risk of bleeding and hemosiderin deposition, explaining the associated hyperpigmentation seen in this patient.
- Insulin injected into LH areas demonstrates delayed onset, reduced peak effect, and increased variability, thereby predisposing patients to alternating hypoglycaemia and hyperglycaemia.
Management
| Immediate cessation of injections in the periumbilical region. |
| Structured site rotation to unaffected areas (lateral abdomen, anterior thighs, and upper arms). |
| Strict single-use of needles/syringes, with education on appropriate disposal. |
| Initial insulin dose reduction of 10–20%, recognizing that insulin bioavailability increases when injections are shifted from lipohypertrophic to normal tissue.⁶ |
| Local skin care with ceramide-based emollients to support barrier repair and gradual resolution of post-inflammatory pigmentation. |
| Diabetes educator-led retraining on injection angle, depth, rotation grids, and needle-change protocol. |
| Close glucose monitoring for the first 3–5 days after site change. |
Follow Up
- Within days of implementing these measures, the patient experienced marked improvement in glycaemic stability, with resolution of unexplained hypoglycaemia and reduced post-prandial excursions.
Discussion
- This case exemplifies a severe yet preventable complication of insulin therapy. Evidence consistently demonstrates that injecting into LH areas increases glycaemic variability and hypoglycaemic risk, often prompting inappropriate insulin dose escalation. Needle reuse—common in resource-limited settings—significantly increases the risk of LH and local tissue injury.
- Routine visual inspection and palpation of injection sites is a low-cost, high-yield clinical practice that can immediately identify this reversible cause of poor glycaemic control. International injection-technique guidelines emphasize site rotation, single-use needles, and regular reassessment of patient technique as standards of care.
CME INDIA Learning Points
| Unexplained glycaemic variability (recurrent hypoglycaemia with post-prandial hyperglycaemia) should immediately prompt inspection of insulin injection sites. |
| Exclusive use of a single injection site—particularly the periumbilical region—strongly predisposes to lipohypertrophy and erratic insulin absorption. |
| Needle or syringe reuse accelerates tissue microtrauma, inflammation, and fibrosis, worsening lipohypertrophy and contributing to post-inflammatory hyperpigmentation. |
| Well-demarcated, indurated, hyperpigmented plaques at injection sites are clinical markers of advanced lipohypertrophy, sometimes with central lipoatrophy. |
| Insulin injected into lipohypertrophic tissue has delayed onset, reduced peak action, and highly variable bioavailability, leading to alternating hypo- and hyperglycaemia. |
| Shifting injections from affected to normal tissue often increases insulin bioavailability; an initial 10–20% dose reduction is prudent to prevent hypoglycaemia. |
| Structured site rotation (lateral abdomen, thighs, upper arms) is a cornerstone of preventing lipohypertrophy and maintaining predictable insulin kinetics. |
| Single-use needles/syringes are not optional: reuse significantly increases local tissue injury, bleeding, and pigmentary change, and compromises glycaemic control. |
| Routine visual inspection and palpation of injection sites is a low-cost, high-yield intervention that can rapidly identify a reversible cause of “insulin failure.” |
| Targeted retraining by diabetes educators—covering rotation grids, injection depth, angle, and needle change—can produce rapid stabilization of glucose profiles within day. |
References:
- Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-453.
- Frid AH, Hirsch LJ, Menchior AR, Morel DR, Strauss KW. Worldwide injection technique questionnaire study: injecting complications and the role of the professional. Mayo Clin Proc. 2016;91(9):1224-1230.
- Frid AH, Hirsch LJ, Gaspar R, et al. New insulin delivery recommendations. Mayo Clin Proc. 2010;85(12 Suppl):S3-S14.
- Young RJ, Hannan WJ, Frier BM, Steel JM, Duncan LJP. Diabetic lipohypertrophy delays insulin absorption. Diabetes Care. 1984;7(5):479-480.
- Gibney MA, Arce CH, Byron KJ, Hirsch LJ. Skin and subcutaneous adipose layer thickness in adults with diabetes at insulin injection sites. Curr Med Res Opin. 2010;26(6):1519-1530.
- Famulla S, Hövelmann U, Fischer A, et al. Insulin injection into lipohypertrophic tissue: blinded and randomized controlled trial. Diabetes Care. 2016;39(9):1486-1492.
- Johansson UB, Amsberg S, Hannerz L, et al. Impaired absorption of insulin aspart from lipohypertrophic injection sites. Diabetes Care. 2005;28(8):2025-2027.
- Kreugel G, Keers JC, Kerstens MN, Wolffenbuttel BH. Influence of needle length on insulin injection. Diabetes Care. 2011;34(12):2525-2530.
- Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations: update on injection technique. Diabetes Metab. 2016;42(4):273-286.
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs