
CME INDIA Presentation by Dr. Kamaldeep Chawla, MD, DNB CARD, FRCP Ed, DM Sc, Sr. Interventional Cardiologist, Vadodara.
56-year-old male with hypertension and pre-diabetes is referred to you after a CAC scan shows a score of 400.
Medications: Metformin Ramipril, No Family Hx of premature CVD
| A1C 6.2% BP 130/82 |
| BMI 29 kg/m2 |
| TC 218 mg/dL |
| LDL-C 102 mg/dL |
| HDL-C 42 mg/dL |
| TG 380 mg/dL |

CAC Scan
How would you treat this patient?
- Lifestyle therapy only.
- Low intensity statin.
- Moderate Intensity statin and aspirin.
- Intensive lifestyle, high intensity statin to achieve LDL< 70 mg/dL, aspirin, add anti- hypertensive therapy, consider GLP1RA.

Clinical Use for CAC Testing in 2025
| Selected intermediate risk patients in whom there is uncertainty about role of statin therapy (Class 2a) |
| Statin averse / intolerant |
| Low risk patients with significant risk factors (e.g., systemic inflammatory disease, Lp(a), strong Fam Hx) |
| Intermediate and high-risk patients in whom intensity of therapy may be uncertain |
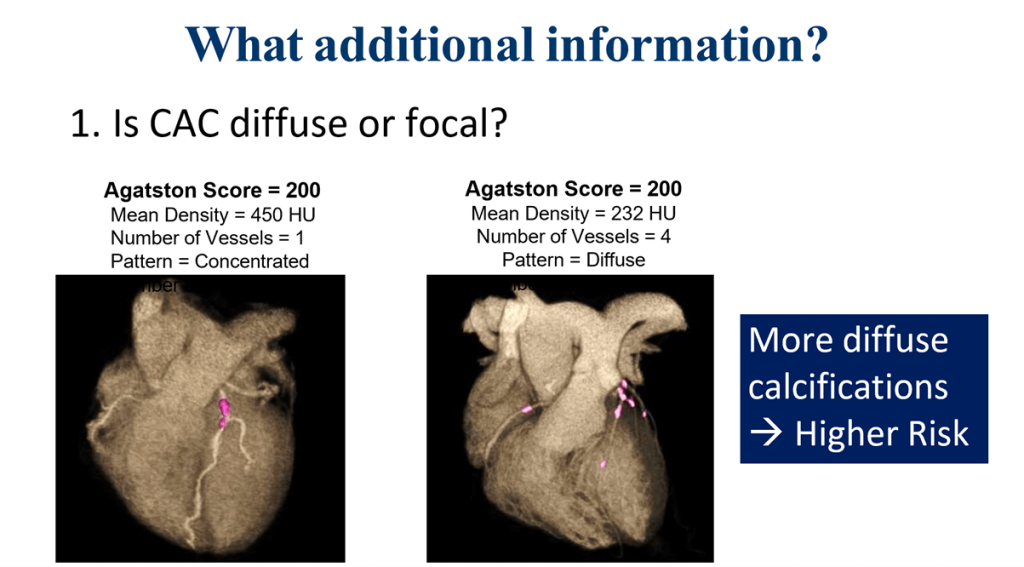
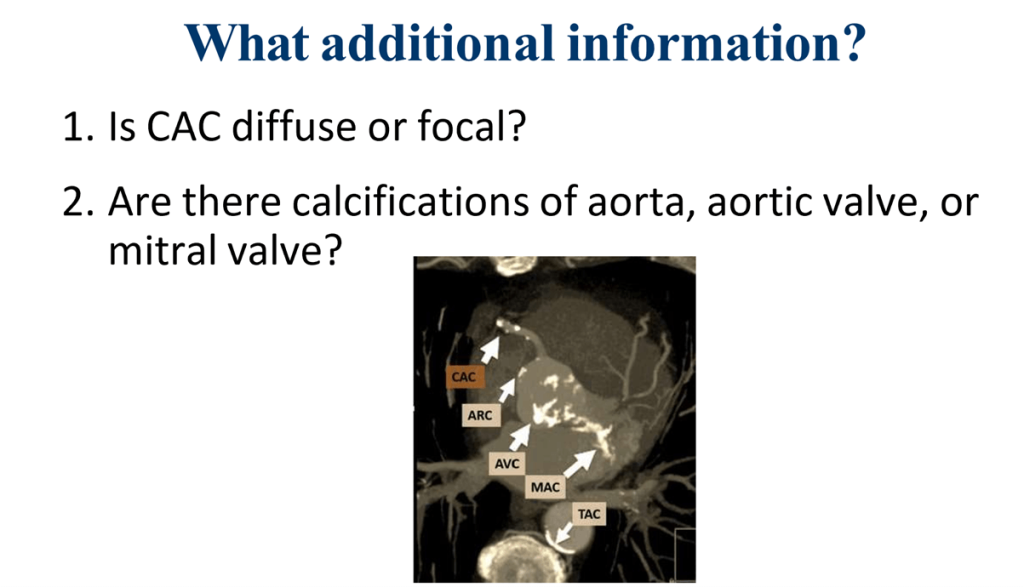
Questions to address when seeing a patient with elevated CAC
- Are there additional imaging or clinical risk factors that inform risk / treatment?
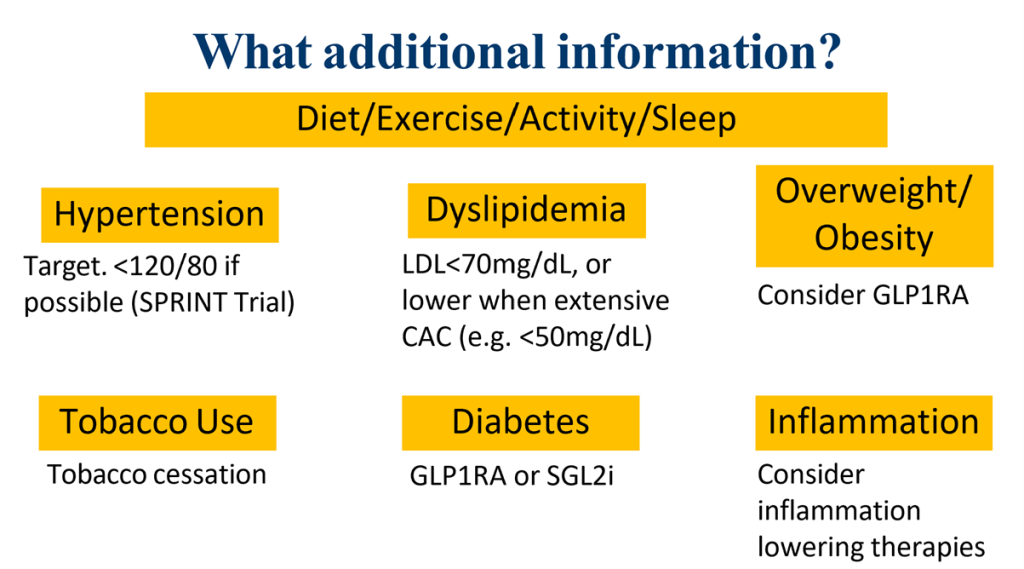
- What preventive therapies should I implement?
- When is additional testing required?
Blood pressure lowering among individuals at risk of CVD (SPRINT Trial)
“Among patients at high risk for cardiovascular events but without diabetes, targeting a systolic blood pressure of less than 120 mm Hg, as compared with less than 140 mm Hg, resulted in lower rates of fatal and nonfatal major cardiovascular events and death from any cause, although significantly higher rates of some adverse events were observed in the intensive-treatment group.”
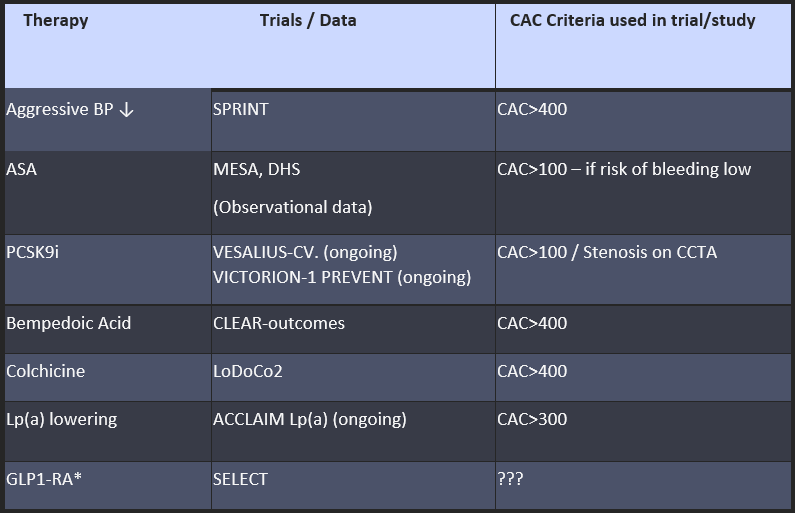
Aggressive Medical Therapy for CAD: Expanding evidence based on CAC
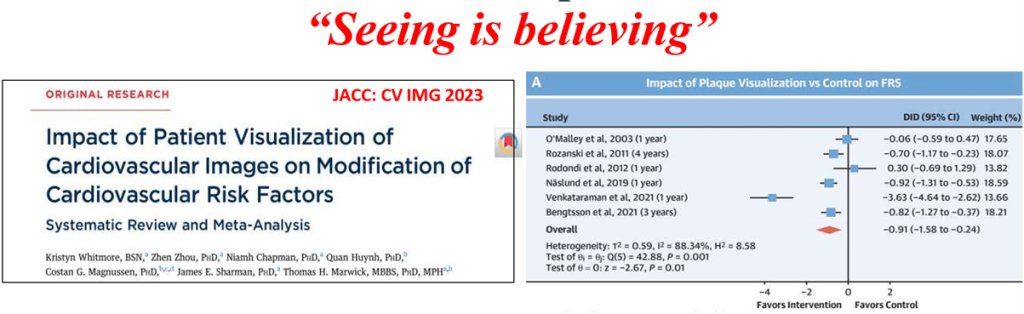
Can we use CAC to improve adherence?
- Patient visualization of CV imaging is associated with overall CV risk reduction and improvement of individual risk factors: cholesterol and systolic blood pressure.
Tips for Showing Images to Patients
| Open and show images in clinic. |
| Use terminology that patients understand: “Plaque” instead of “Calcifications.” |
| Share that atherosclerosis is common…they are not that unique. |
| Emphasize preventive aspects – CVD events are preventable! |
| Avoid temptation to repeat imaging to assess response! |
| No role for repeat CAC once significant plaque identified. |
Not all patients with high CAC have same risk
Risk may be relatively LOWER if:
- High exercise capacity
- Absence of risk factors
When is more testing needed after CAC?
- Answer: Rarely!
- If patient has high exercise capacity and is asymptomatic no further testing needed! (Focus on preventive therapies instead).
- If uncertainty about exercise capacity / symptoms → ETT.
- When very high risk (e.g., CAC>1000) and possible symptoms, stress may be reasonable. (PET>Stress MRI>Stress echo>SPECT); CCTA an option if photon counting CT.
- Invasive angiography never recommended.
CME INDIA Learning Points
By Dr. Kamaldeep Chawla
| Patients with elevated CAC have increased risk. |
| Intensity of preventive measures based on amount of CAC & other risk factors: |
| • Lifestyle therapies for all. |
| • LDL lowering |
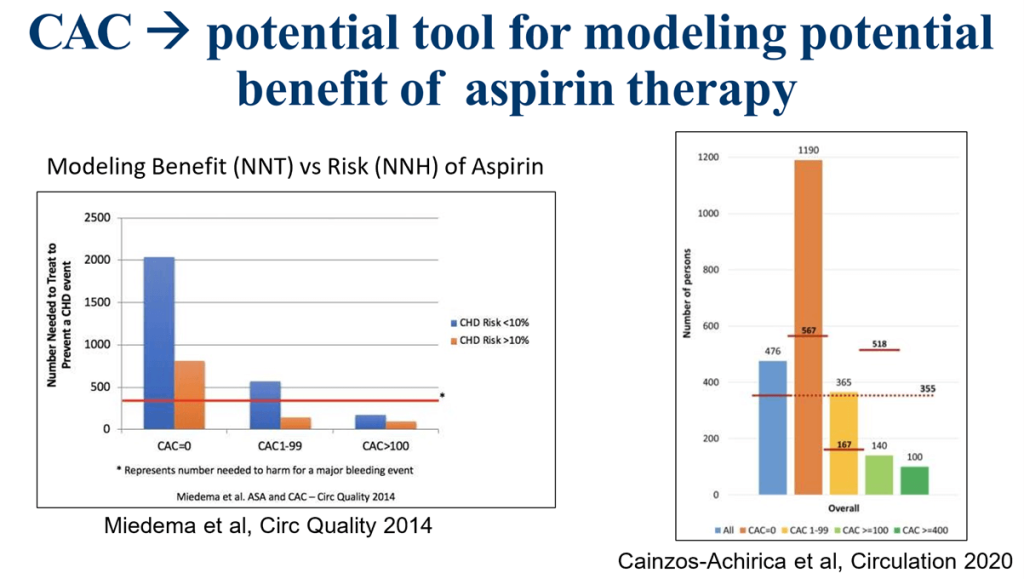
| • Consider ASA if severe CAC AND low risk of bleeding, based on discussion. |
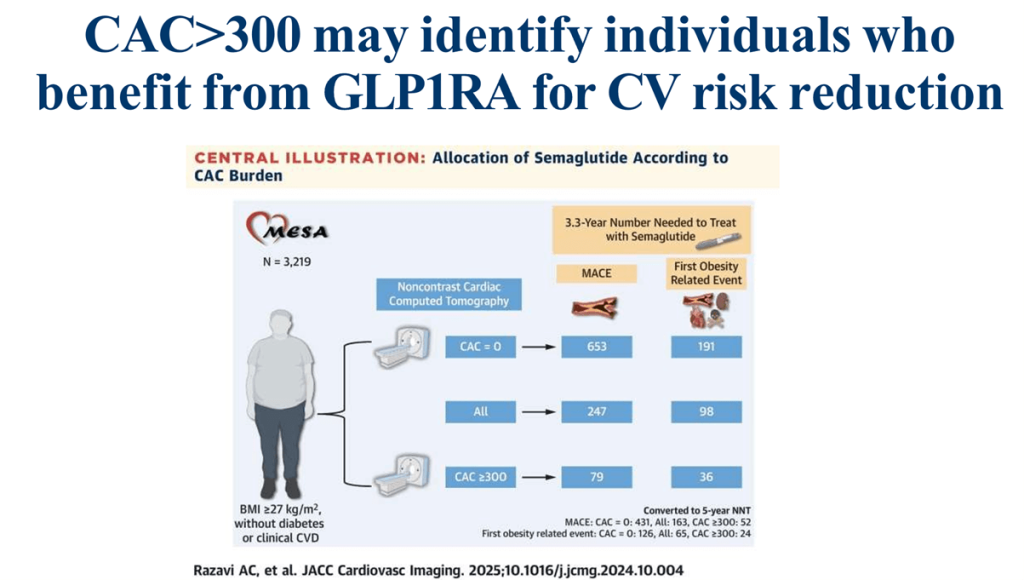
| • GLP1RA if overweight/DM. |
| • BP control. |
| No further testing required if asymptomatic. |
| If uncertain regarding symptoms → ETT. |
| If stress test → exercise preferred unless PET with quantitative MBFR if available. |
CME INDIA Clinical Pearls
Role of Coronary Artery Calcium (CAC) Scoring in CAD Risk Stratification
Who should get a CAC scan?
- Patients > 40 years with one or more CAD risk factors
- Individuals with stable angina symptoms
- Those in the borderline to intermediate ASCVD risk category
- Cases where traditional risk tools give uncertain guidance
Clinical utility of CAC scoring:
- Helps stratify risk and personalize decision-making
- Guides next steps:
→ Revascularization (if high CAC and symptoms)
→ Medical therapy intensification
→ Routine follow-up (if low CAC score)
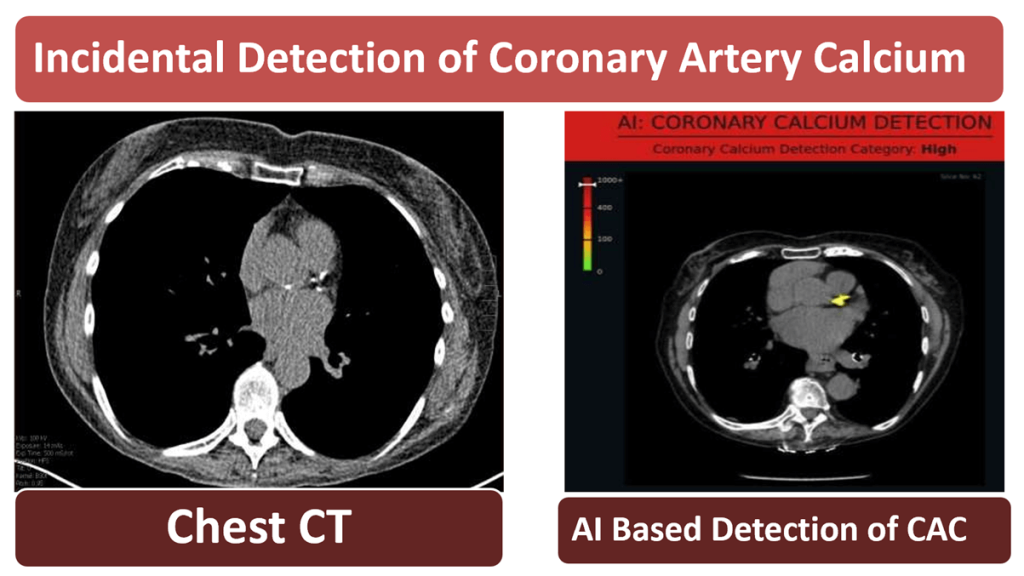
AI and CAC – The Future:
- Artificial Intelligence (AI) can enhance CAC data interpretation
- Offers potential for greater diagnostic accuracy, automation, and individualized risk prediction
CAC vs. Traditional Risk Scores:
- CAC provides direct anatomical evidence of coronary atherosclerosis
- Adds value beyond scores like Framingham or Pooled Cohort Equation
- Especially useful when clinical risk is ambiguous or underestimated by traditional tools
Bottom Line:
- Add CAC scoring to traditional risk models for better CAD evaluation in symptomatic or at-risk individuals
- Safe, quick, and cost-effective
- Enhances patient-specific treatment planning
References:
- https://www.nhlbi.nih.gov/science/systolic-blood-pressure-intervention-trial-sprint-study
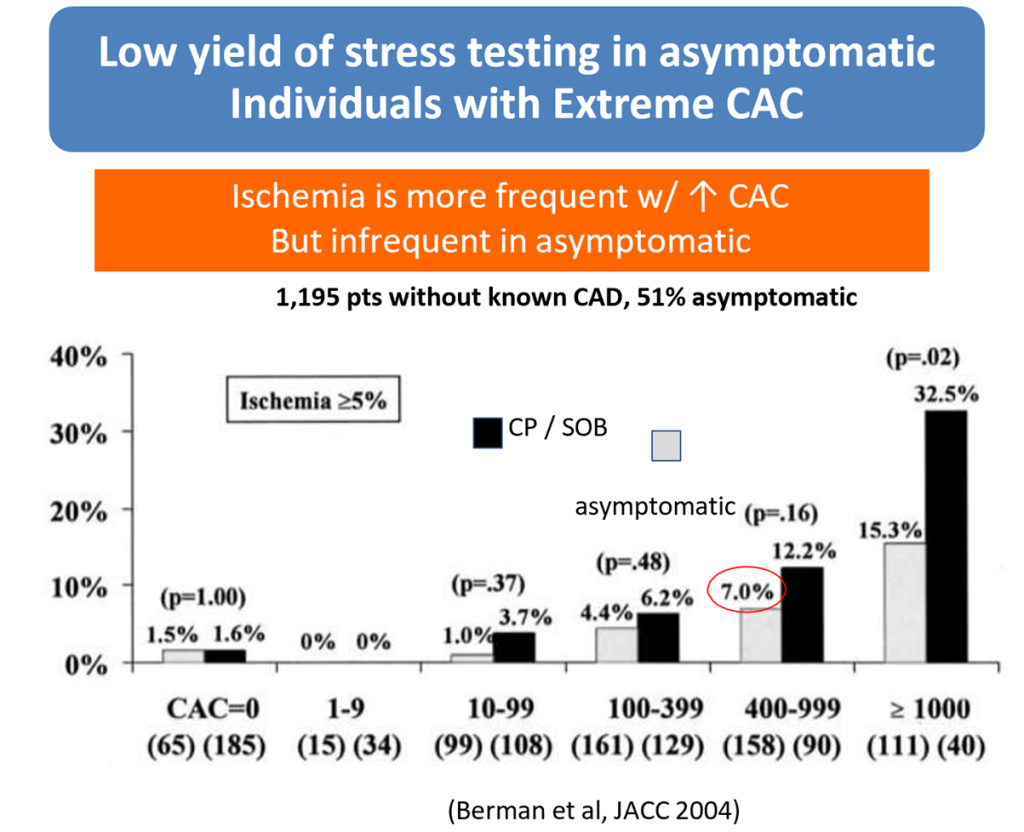
- Berman DS, Wong ND, Gransar H, Miranda-Peats R, Dahlbeck J, Hayes SW, Friedman JD, Kang X, Polk D, Hachamovitch R, Shaw L, Rozanski A. Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography. J Am Coll Cardiol. 2004 Aug 18;44(4):923-30. doi: 10.1016/j.jacc.2004.06.042. PMID: 15312881.
- https://www.jacc.org/journal/imaging
- Rezaie-Kalamtari, K., Norouzi, Z., Salmanipour, A. et al. Updates on CAD risk assessment: using the coronary artery calcium score in combination with traditional risk factors. Egypt Heart J 77, 14 (2025). https://doi.org/10.1186/s43044-025-00608-4
- Razavi AC, et al. JACC Cardiovasc Imaging. 2025;10.1016/j.jcmg.2024.10.004
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs