

CME INDIA Case Presentation by Dr. A. N. Rai, Consultant Physician, Cardiologist, Gaya, Bihar, Bharat
CME INDIA Case Study
How Presented?
- A Middle-aged diabetic female with CKD had PCNL (Percutaneous nephrolithotomy) for large Renal stones 3 days ago.
- She was on Insulin and SGLT2-Inhibitor for control of diabetes and amlodipine and atenolol for Hypertension.
- SGLT2 was stopped 3 days prior to surgery.
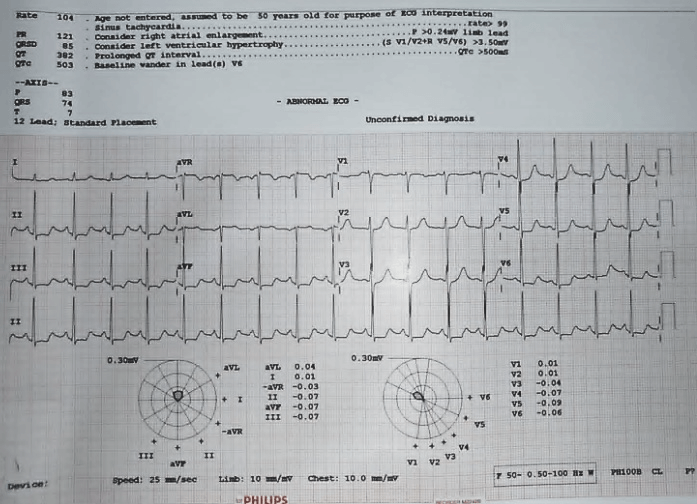
- Her preoperative Blood Chemistry and ECG given below.
- Her condition suddenly deteriorated on 3rd postoperative day with fall of BP 90 mg systolic and severe Bradycardia with pulse rate 50/ minutes.
- Her Blood Chemistry and ECG:
15/6/2024
- Hb-8 gm/dl, TLC-4400 cells/cmm, Platelet count 91000 lakhs/cmm.
- Fasting blood sugar-204 mg/dl.

ECG – 18/06/2024
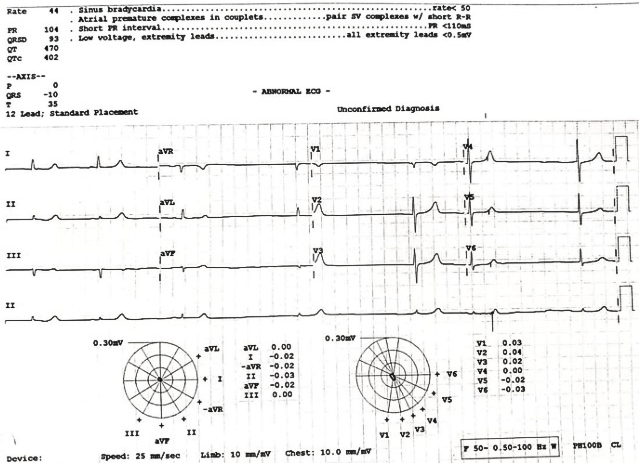
18/06/2024

CME INDIA Comments
Dr. Basab Ghosh, Agartala:
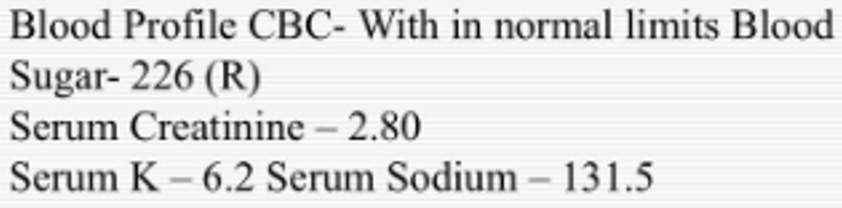
- K-5.1.
- QT prolongation is there.
- Sugar must have been taken care.
- Long-term increase in FBS could be associated with increased risk of sudden cardiac arrest.
Dr. A. N. Rai, Gaya:
- Although Preoperative Blood Sugar was high, but 3 hours before operation it came down to 130 mg and remained between 140 to 180 on post operative period. Echo showed concentric LVH with EF 55%.
Dr. S. K. Goenka, Begusarai:
- Could anaesthetic drugs can cause sudden fall in BP and Pulse, etc in such operative cases? ECG is showing inferolateral Ischaemia.
Dr. Awadhesh K. Singh, Kolkata:
- Tamponade? Cr, TSH baseline?
Dr. Bhanu Pratap Singh, Siwan:
- 2nd ecg showing s bradycardia with low voltage. Serum potassium not corresponding to ECG findings. Echo rules out tamponade.
- D/d hypothermia/Addison disease.
Dr. D. P. Khaitan, Ahmedabad:
- 1st ECG-PROXIMAL LAD.
- New LAD Occlusion pattern “Precordial Swirl,” in which there is rightward STE vector, with STE in V1 and aVR, with reciprocal STD in V5 and V6. It is due to transmural ischemia not only of the anterior wall and apex, but due to transmural ischemia of the septum, usually due to occlusion proximal to the first septal perforator. Later K increased led to Bradycardia.
Dr. U. Kumar:
- Anaemia with CKD, Electrolyte imbalance causing Bradycardia, (B blocker induced).
Dr. Rishad Ahmed, Hyderabad:
- BRASH.
Dr. D. P. Khaitan, Gaya:
- I am also in favour of BRASH Syndrome.
- B = Bradycardia due to different mechanism being operated through at SA Node and AV node
- R = Renal impairment.
- AV nodal blockade drug (The patient might has received B blocker by seeing the 1st ECG).
- S = Shock – clinical history is in its favour
- H = Hyperkalaemia might has further progressed from 5.1 mEq/L
- This has been observed that junctional rhythm with a borderline higher serum K level without heightened T can be observed.
- The patients in shock might have low voltage. Low voltage by itself is very poor prognostic indicator bin term of mortality if associated with acute coronary syndrome orLVF.
Dr. A. Rai Gaya:
- Congratulations to Dr Rishad Ahmad and Dr D P Khaitan for correct diagnosis of BRASH Syndrome.
- This patient has classical features of BRASH Syndrome.
- Bradycardia.
- Renal failure.
- AV Blocker Drug.
- Shock.
- Hyperkalaemia.
- Key features of BRASH Syndrome differentiating it from isolated hyperkalaemia or intoxication from AV node blocking medications.
- The degree of hyperkalaemia is moderate and out of proportion to the observed bradycardia. Typically, isolated hyperkalaemia must be severe (~ 6mEq/L) before causing bradycardia.
- ECG may show bradycardia without other features of hyperkalaemia.
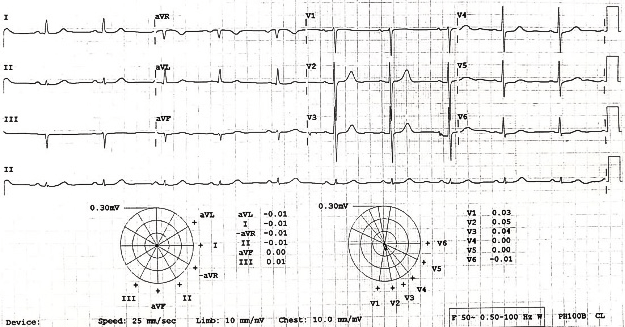
- Patient was managed by IV Atropine stat followed by medical management of Hyperkalaemia by giving IV Insulin and glucose Infusion, IC Calcium and nebulisation . With above treatment improved. B P became normal 130/80. Her ECG and blood Chemistry is given below:
20/06/2024
19/06/2024

Dr. D. P. Khaitan:
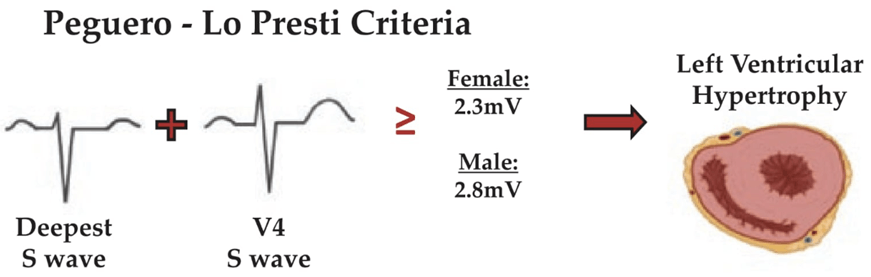
- There is evidence of LVH in both ECG and cardiac echo, therefore Swirl sign is falsely positive in the presence of LVH.
- This is the criteria for LVH estimation on ECG and per formula P-L-P this is about 2.7, more than 2.3 (The patient is female).
- I had a discussion with Respected Dr. A. N. Rai and came to the conclusion:
- On 1st ECG there is pseudo positive swirl sign due to associated LVH.
- The 2nd ECG shows BRASH Syndrome, which has been discussed.
CME INDIA Learning Points
- BRASH syndrome is an acronym for Bradycardia, Renal Failure, AV blockade, Shock, and Hyperkalemia.
- BRASH syndrome results from a synergistic interaction between hyperkalemia and medications that block the atrioventricular (AV) node. The most common triggers are hypovolemia and medications that promote hyperkalemia or cause renal injury.
- At its core, BRASH syndrome is driven by the interplay between hyperkalemia and AV node-blocking medications. This syndrome lies on a spectrum, ranging from isolated hyperkalemia to an overdose of an AV nodal blocking medication, such as beta-blockers.
- Understanding and recognizing BRASH syndrome as a distinct entity, as discussed by Farkas et al. in 2020, can lead to improved patient outcomes. Treatment includes fluid resuscitation, therapies for hyperkalemia (such as intravenous calcium, insulin/glucose, beta agonists, and diuretics), and management of bradycardia.
- The potential population at risk for developing BRASH syndrome is very large.
- Patients with BRASH syndrome may present with a variety of symptoms, ranging from asymptomatic bradycardia to multiorgan failure.
- The most common presentation starts with hypovolemia due to factors such as gastrointestinal illness. This hypovolemia causes poor kidney perfusion, leading to acute kidney injury, which impairs the normal excretion of AV blocking drugs and potassium. The accumulation of AV blocking drugs causes bradycardia and shock, further worsening kidney perfusion and establishing a positive feedback loop.
- Recognizing the constellation of clinical findings and managing BRASH syndrome as a whole is crucial, rather than treating individual factors in isolation. Standard ACLS algorithms without calcium may lead to unnecessary interventions such as transvenous pacemakers. Breaking the cycle of BRASH syndrome involves:
- Calcium: For moderate to severe hyperkalemia, calcium stabilizes the myocardium, potentially improving heart rate and cardiac output.
- Fluid Resuscitation: Most patients with BRASH syndrome are volume-depleted. A suitable fluid is ‘normal’ bicarbonate, made by adding 150 ml of 8.4% sodium bicarbonate to 850 ml of water for injection, resulting in 1 liter of isotonic fluid. However, assess fluid status individually as some patients may develop oliguric renal failure, fluid retention, and volume overload.
- Enhancing Potassium Excretion: Diuresis with potassium-wasting diuretics such as furosemide, or dialysis if the patient is anuric.
- Adrenaline: If calcium fails to resolve bradycardia, adrenaline can increase heart rate, cardiac output, and renal perfusion, and shift potassium intracellularly, improving hyperkalemia. Isoprenaline is an alternative chronotropic agent, preferred over beta-agonists like dobutamine or dopamine.
- Key Considerations:
- Avoid focusing on a single component of the syndrome, such as hyperkalemia, and overlooking other aspects like hypovolemia and bradycardia.
- If the patient remains shocked despite being euvolemic, inotropes like adrenaline may be necessary due to their chronotropic and vasoconstrictive properties.
- Patients with BRASH syndrome often have a higher baseline blood pressure due to their underlying conditions.
- Consider other temporizing treatments for hyperkalemia such as insulin/dextrose and salbutamol.
CME INDIA Tail-Piece
Echo-CAD, RWMA RCAEF-40%
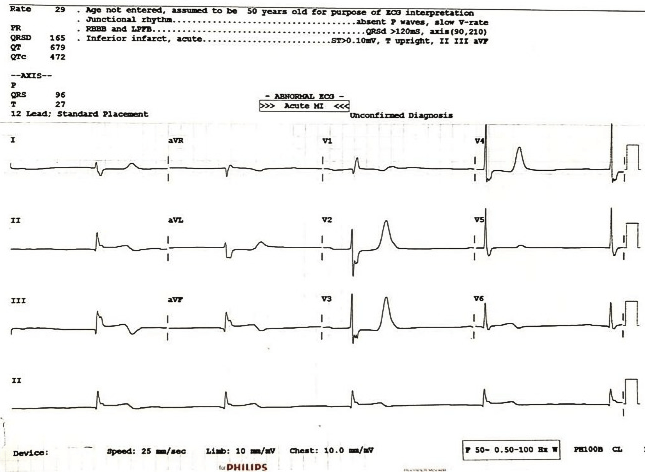
Dr. Parvesh: Inferior wall infarct with complete heart block.
Dr. Sudha: Inferior wall mi with a complete heart block. Stokes Adams maybe.
Dr. U. Kumar: Looks inferior mi with posterior MI but q wave in lead v1 against posterior MI. Tiny q wave in inferior leads (Not significant) and prolonged ST may against IWMI. Why there is j point notching? Basically, the convulsions are due to Stokes Adam syndrome.
Dr. D. P. Khaitan:
- Acute Inferior myocardial infarction with ST segment elevation more over Lead III compared with other leads – RCA involvement.
- There is Tall T over chest leads V2 -V4 with definite ST depression over V2.
- Plus, Mild ST elevation with small R over V6 – All these indicate the possibility of Acute Posterior Myocardial infarction as well. Since V6 is the forward extension to leads V7-8 which must be recorded in such a case.
- There are three sets of conduction disturbances:
- RBBB (please see the terminal negative wide/deep wave S in lead 1 which is associated with RBBB).
- Left posterior hemiblock = Bifscicular block.
- Superimposed upon Junctional rhythm = Stokes Adams Syndrome.
Dr. A. N. Rai:
- ECG shows Acute Inferior STEMI with severe Bradycardia and absent P wave therefore it is not a complete Heart Block but due to Nodal Bradycardia. Tall T wave in Precordial leads
- ( V1 to V4) is due to Hyperkalaemia. Blood chemistry and Echo of the patient is given below
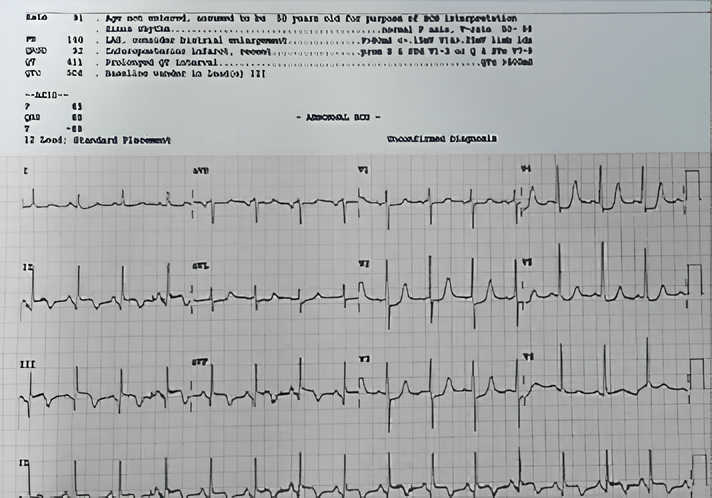
- After successful medical management of Acute Inferior STEMI and Hyperkalaemia patient improved . ECG and Blood Chemistry after recovery is given below.

Further Readings:
- McLaren J. ECG Cases 10 – Hyperkalemia: The Great Imitator. Emergency Medicine Cases. 2020
- Helman A. 4-Step Approach to Bradycardia and Bradydysrhythmias. Emergency Medicine Cases. 2021
- McLaren J. ECG Cases 20 – Approach to Bradycardia and the BRADI Mnemonic. Emergency Medicine Cases. 2021
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
How to contribute or ve indiscussion
Professor of pharmacology and consultant