
CME INDIA Presentation by Dr. Kalyan Kumar Gangopadhyay, MD, MRCP, FRCP, CCST, CMRI, Peerless Hospitals, Kolkata.
Based on presentation at DTECON-2024, Jaipur, Bharat.
What is Sarcopenic obesity?
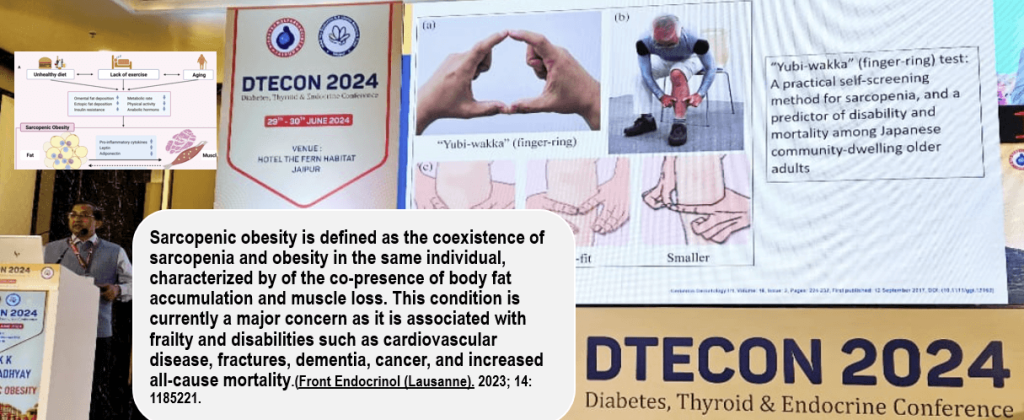
- Sarcopenic obesity is defined as the coexistence of sarcopenia and obesity in the same individual. The lack of universally accepted criteria for defining sarcopenic obesity hinders precise epidemiological assessment, proper patient identification, and tailored management to mitigate associated complications. A meta-analysis of 50 studies involving 86,285 people found that the global prevalence of sarcopenic obesity in individuals over 60 years old is 11%.
Learning about Muscle and Muscle loss

Definitions of Body Composition Compartments
Sarcopenic Obesity: Simplified

Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment
- The Asian Working Group for Sarcopenia (AWGS) 2014 consensus defined sarcopenia as “age-related loss of muscle mass, plus low muscle strength, and/or low physical performance” and specified cutoffs for each diagnostic component.

- Low muscle strength is defined as handgrip strength less than 28 kg for men and less than 18 kg for women. Criteria for low physical performance include a 6-meter walk at less than 1.0 m/s, a Short Physical Performance Battery (SPPB) score of 9 or lower, or taking 12 seconds or more for the 5-time chair stand test. The AWGS 2019 guidelines retain the original cutoffs for height-adjusted muscle mass: for dual-energy X-ray absorptiometry, less than 7.0 kg/m² in men and less than 5.4 kg/m² in women; for bioimpedance, less than 7.0 kg/m² in men and less than 5.7 kg/m² in women.
- Additionally, the AWGS 2019 update introduces separate algorithms for community versus hospital settings. Both algorithms begin by screening either calf circumference (less than 34 cm in men, less than 33 cm in women), SARC-F (a score of 4 or higher), or SARC-CalF (a score of 11 or higher) to facilitate earlier identification of individuals at risk for sarcopenia. While skeletal muscle strength and mass remain crucial for a definitive clinical diagnosis, AWGS 2019 also introduces the concept of “possible sarcopenia.” This is defined by either low muscle strength or low physical performance alone and is intended for use in primary health care or community-based health promotion to enable earlier lifestyle interventions.
- Although defining sarcopenia by body mass index (BMI)-adjusted muscle mass rather than height-adjusted muscle mass might better predict adverse outcomes, more evidence is needed before changing the current recommendations. Lifestyle interventions, especially exercise and nutritional supplementation, continue to be the mainstays of treatment. Further research is required to investigate the potential long-term benefits of lifestyle interventions, nutritional supplements, or pharmacotherapy for sarcopenia in Asians.
An elusive consensus definition of sarcopenia impedes research and clinical treatment: A narrative review(2023)
- The definition of sarcopenia, the age-related loss of muscle mass, has evolved over time, yet there remains no consensus. Various definitions of sarcopenia typically focus on the loss of muscle mass, loss of function, and weakness. Common criteria include appendicular lean soft tissue mass (often referred to as muscle mass), grip strength, and gait speed. However, there is still a lack of agreement on operational definitions and diagnostics for this condition, which may be due to the absence of appropriate tools that accurately measure relevant outcomes, such as skeletal muscle rather than lean mass.
- 2023 consensus describes the evolution of the consensus groups’ definition of sarcopenia, highlight the need for more accurate measures of muscle mass and function, and discuss effective, low-cost treatments such as resistance training and diet. Achieving consensus on the definition of sarcopenia is crucial for advancing research in the field and for understanding the prognostic value of a sarcopenia diagnosis and the appropriate treatment for patients.

Existing tools and their utility for the assessment of sarcopenia
- The choice of measurement tools and cutoff points is critical. A cutoff that underestimates prevalence leads to underdiagnosis and undertreatment, while a cutoff that overestimates prevalence may result in overtreatment (Vellas et al., 2018). Therefore, it is essential that prognostic criteria accurately measure the outcome of interest and that valid and reliable cutoffs are selected to accurately capture and diagnose individuals with sarcopenia.


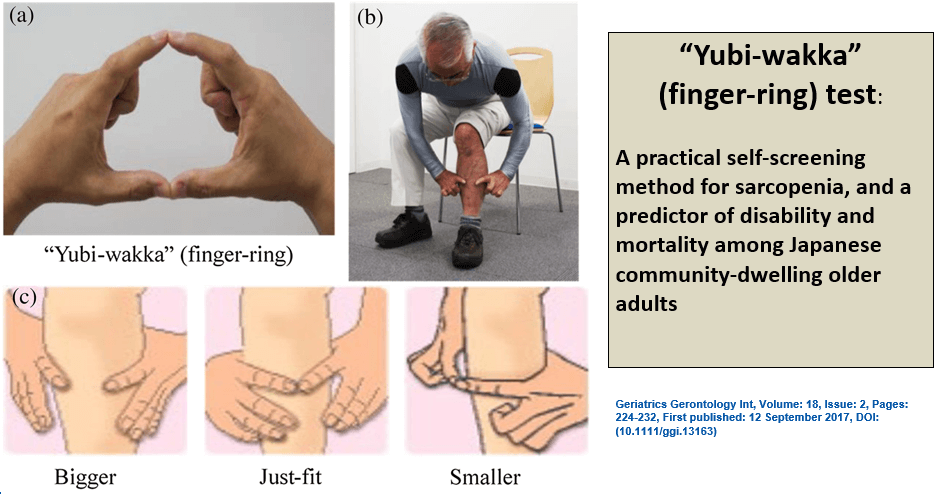
“Yubi-wakka” (finger-ring) test: A practical self-screening method for sarcopenia, and a predictor of disability and mortality
- The “Yubi-wakka” test is a practical method to identify older adults at risk of sarcopenia, disability, and mortality. It may contribute to increased primary prevention for sarcopenia by serving as an early alert for older adults against becoming sarcopenic.
- The “Yubi-wakka” test is a simple method to assess sarcopenia. It involves three steps:
- Make a ring using the index fingers and thumbs of both hands.
- Gently circle the thickest part of the non-dominant calf, which is bent at a 90° angle.
- Check if the non-dominant calf circumference is “bigger,” “just fits,” or “smaller” compared to the finger-ring circumference.
- The test is performed with the participant seated and does not require any instruments.
Bio-electrical impedance analysis
- Though BIA is less expensive than DXA, its reliability is compromised at a BMI greater than 35 kg/m², making it less useful in cases of sarcopenic obesity.
- Bioelectric impedance analysis (BIA) is quick, noninvasive, and relatively inexpensive, making it ideal for bedside use. However, BIA assumes static ratios, notably a fixed hydration of tissues, which often do not apply to critically ill patients, complicating interpretation. Despite this, exploring potential applications is worthwhile, as BIA currently appears to be the most feasible body composition measurement technique in the ICU
Sarcopenic obesity and Calcium scoring
- A retrospective observational study included subjects who underwent routine health check-ups at Seoul National University Hospital between January 2017 and December 2018. The study found that 9.5% had sarcopenia, 40.7% were obese, and 8.4% had sarcopenic obesity (SO).
Sarcopenic obesity and CVD
- While some studies suggest that sarcopenic obesity may have weak or no links to cardiovascular disease (CVD), recent cross-sectional and cohort studies indicate that sarcopenic obesity, when measured by muscle strength rather than muscle mass, is associated with increased risks of CVD and cardiovascular mortality. Additionally, recent research has shown an independent correlation between sarcopenic obesity and coronary artery calcification.
Which is more important – muscle mass or weakness?
- Sarcopenic-obesity, based on muscle strength but not muscle mass, was modestly associated with increased CVD risk. These findings imply that strength may be more important than muscle mass for CVD protection in old age.(Ref-9)
The Impact of Glucose-Lowering Drugs on Sarcopenia in Type 2 Diabetes

- It is well established that insulin can reduce the risk of sarcopenia, while DPP-4 inhibitors (DPP-4i) might have a neutral impact on it. Data on other glucose-lowering drugs remain controversial and inconclusive.
- However, emerging evidence indicates that treatment with SGLT2 inhibitors (SGLT2i) may contribute to a reduction in skeletal muscle index (SMI) and skeletal muscle mass (SMM). These adverse effects of SGLT2i on muscle contrast with the multiple beneficial effects of this drug on other common diabetes complications affecting the kidney and the heart.
- It seems appropriate to consider limiting the use of SGLT2 inhibitors (SGLT2i) in elderly patients with sarcopenia or at high risk for this condition, unless other clinical conditions justify their use.
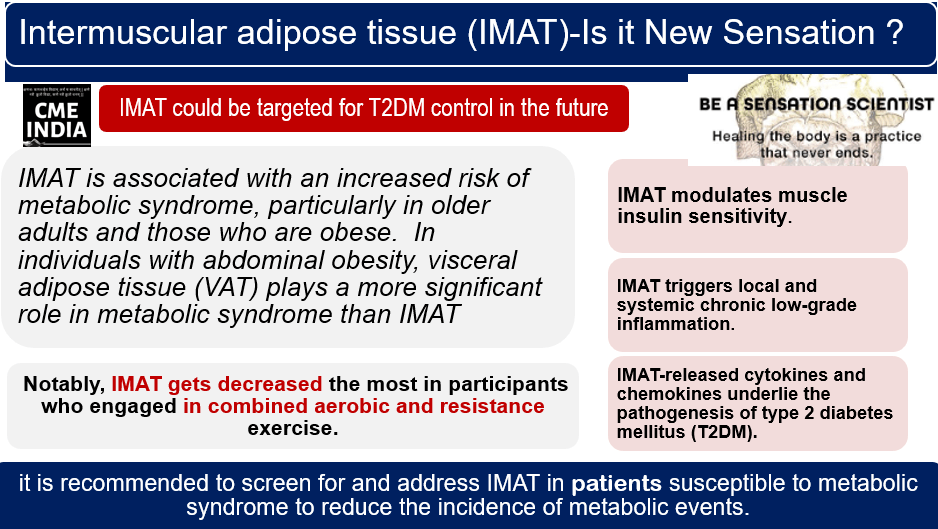
Intermuscular adipose tissue:

| Intermuscular adipose tissue (IMAT) is defined as adipose tissue interspersed between and around skeletal muscle groups. |
| Intermuscular adipose tissue (IMAT) is a distinct type of fat depot that is strongly associated with insulin resistance, type 2 diabetes mellitus, and aging. Intermuscular adipose tissue (IMAT) affects the local muscle microenvironment by increasing interstitial free fatty acids (FFAs), which promotes muscle insulin resistance. IMAT lipolysis can alter the local interstitial concentration of FFAs without changing systemic fatty acid levels, effectively concealing the impact of IMAT on the muscle microenvironment from detection in the systemic circulation. |
| Although IMAT constitutes a relatively small proportion of the body’s total adipose and subcutaneous tissue, its overall quantity can be comparable to that of abdominal visceral adipose tissue. |
| The molecular, cellular, and other biological characteristics of IMAT are still being explored and understood. |
| IMAT originates from at least three distinct cell types. |
| Gaining access to human IMAT samples through biopsies, along with advanced molecular biology techniques such as transcriptomics, proteomics (including single-cell or single-nuclei sequencing), and secretome (exosomes) analyses, will be essential for a deeper understanding of the role of this unique adipose tissue in human health and disease. |
| Diagnosing intermuscular adipose tissue (IMAT) typically involves imaging techniques such as MRI (Magnetic Resonance Imaging) or CT (Computed Tomography) scans. These methods enable the visualization of fat deposits within and around muscles. IMAT is quantified by measuring the fat content in specific muscle regions. If you suspect IMAT-related issues, consult a healthcare professional for accurate assessment and guidance. |
CME INDIA Quick Take Away
| Sarcopenic obesity underrecognized but serious entity |
| Problems with clear diagnostic criteria |
| More studies needed; prognostic significance |
| Antidiabetic agents |
| Exercise especially resistance |
CME INDIA Tail-Piece
References:
- Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, Jang HC, Kang L, Kim M, Kim S, Kojima T, Kuzuya M, Lee JSW, Lee SY, Lee WJ, Lee Y, Liang CK, Lim JY, Lim WS, Peng LN, Sugimoto K, Tanaka T, Won CW, Yamada M, Zhang T, Akishita M, Arai H. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc. 2020 Mar;21(3):300-307.e2. doi: 10.1016/j.jamda.2019.12.012. Epub 2020 Feb 4. PMID: 32033882.
- Wei S, Nguyen TT, Zhang Y, Ryu D, Gariani K. Sarcopenic obesity: epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Front Endocrinol (Lausanne). 2023 Jun 30;14:1185221. doi: 10.3389/fendo.2023.1185221. PMID: 37455897; PMCID: PMC10344359.
- Liu X, Ma C, Wang S, Liang Z, Yang J, Zhou J, Shu Y, He Z, Zong J, Wu L, Peng P, Su Y, Gao M, Shen K, Zhao H, Ruan J, Ji S, Yang Y, Tang T, Yang Z, Luo G, Zeng M, Zhang W, He B, Cheng X, Wang G, Wang L, Lyu L. Screening of osteoporosis and sarcopenia in individuals aged 50 years and older at different altitudes in Yunnan province: Protocol of a longitudinal cohort study. Front Endocrinol (Lausanne). 2022 Nov 14;13:1010102. doi: 10.3389/fendo.2022.1010102. PMID: 36452328; PMCID: PMC9704050.
- Coletta G, Phillips SM. An elusive consensus definition of sarcopenia impedes research and clinical treatment: A narrative review. Ageing Res Rev. 2023 Apr;86:101883. doi: 10.1016/j.arr.2023.101883. Epub 2023 Feb 13. PMID: 36792012.
- Vellas, Bruno, et al. “Implications of ICD-10 for sarcopenia clinical practice and clinical trials: report by the international conference on frailty and sarcopenia research task force.” The Journal of frailty & aging 7 (2018): 2-9.
- Tanaka T, Takahashi K, Akishita M, Tsuji T, Iijima K. “Yubi-wakka” (finger-ring) test: A practical self-screening method for sarcopenia, and a predictor of disability and mortality among Japanese community-dwelling older adults. Geriatr Gerontol Int. 2018 Feb;18(2):224-232. doi: 10.1111/ggi.13163. Epub 2017 Sep 12. PMID: 28898523.
- Moonen HPFX, Van Zanten ARH. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness. Curr Opin Crit Care. 2021 Aug 1;27(4):344-353. doi: 10.1097/MCC.0000000000000840. PMID: 33967207; PMCID: PMC8270506.
- Zhang X, Xie X, Dou Q, Liu C, Zhang W, Yang Y, Deng R, Cheng ASK. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: a updated meta-analysis. BMC Geriatr. 2019 Jul 3;19(1):183. doi: 10.1186/s12877-019-1195-y. PMID: 31269909; PMCID: PMC6610788.
- W.C. Stephen, I. Janssen,Sarcopenic-obesity and cardiovascular disease risk in the elderly,The Journal of nutrition, health and aging,Volume 13, Issue 5,2009,Pages 460-466,ISSN 1279-7707,https://doi.org/10.1007/s12603-009-0084-z.
- Massimino E, Izzo A, Riccardi G, Della Pepa G. The Impact of Glucose-Lowering Drugs on Sarcopenia in Type 2 Diabetes: Current Evidence and Underlying Mechanisms. Cells. 2021 Aug 1;10(8):1958. doi: 10.3390/cells10081958. PMID: 34440727; PMCID: PMC8393336.
- Goodpaster, B.H., Bergman, B.C., Brennan, A.M. et al. Intermuscular adipose tissue in metabolic disease. Nat Rev Endocrinol 19, 285–298 (2023). https://doi.org/10.1038/s41574-022-00784-2
- Suka Aryana IGP, Paulus IB, Kalra S, Daniella D, Kuswardhani RAT, Suastika K, Wibisono S. The Important Role of Intermuscular Adipose Tissue on Metabolic Changes Interconnecting Obesity, Ageing and Exercise: A Systematic Review. touchREV Endocrinol. 2023 May;19(1):54-59. doi: 10.17925/EE.2023.19.1.54. Epub 2023 May 17. PMID: 37313233; PMCID: PMC10258613.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs