
CME INDIA Case Presentation Dr. Ravishankar Dwivedi, Consultant Dermatologist, Ranchi, Jharkhand, Bharat.
CME INDIA Case Study
- Dermatology is all about pictures and visuals
- Sometimes a small intervention makes a dramatic impact in the patient’s life
How Presented?
- A 6-year-old child from rural Chhattisgarh.
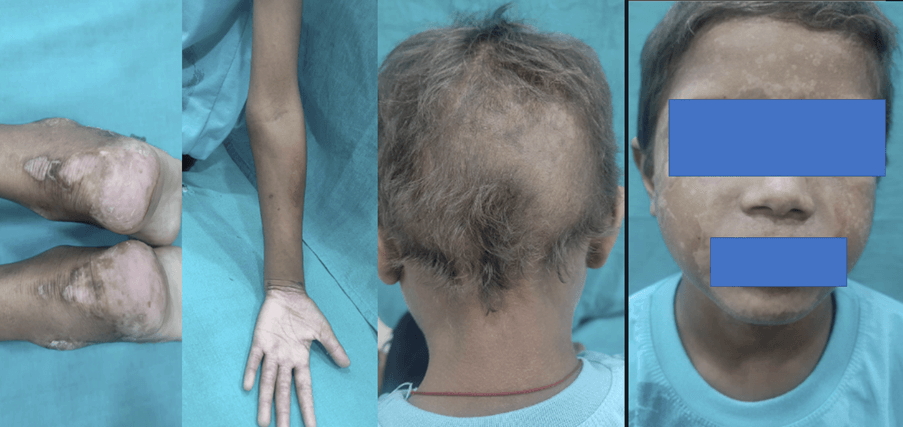
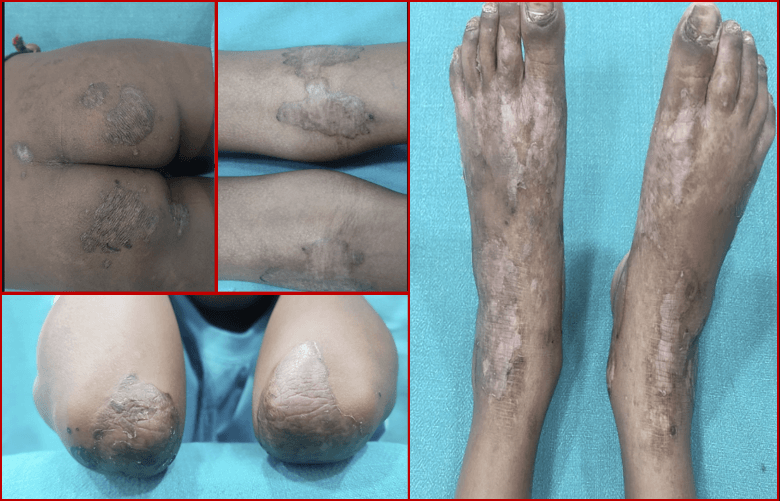
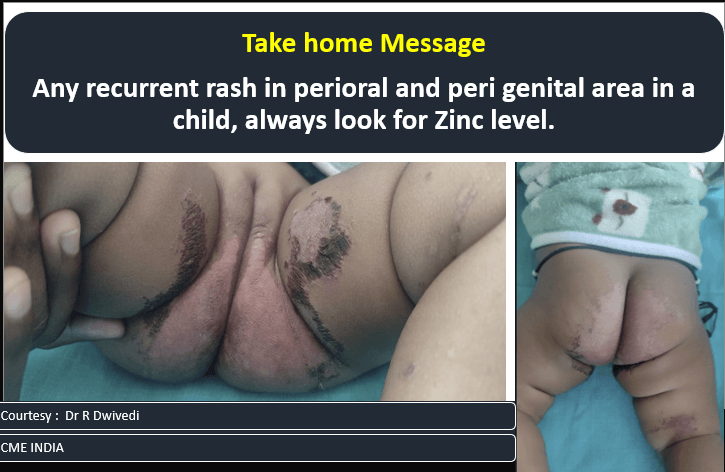
- Has a history of recurrent painful encrusted lesions on extremities, pressure points, scalp, ano-genital area, and face.
- Treated multiple times since childhood, responding to medication prescribed by general practitioners or pediatricians, but the lesions invariably recur.
Clinical Pictures: What they tell?
1.

2.

3.

What Clinched the Diagnosis?
- High level of suspicion seeing above pics
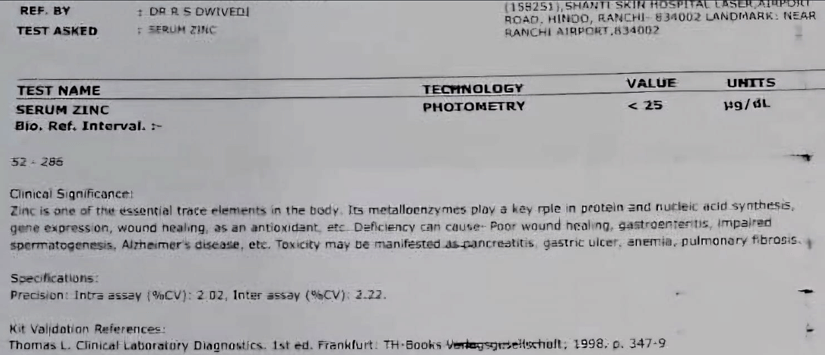
- Estimation of serum Zinc level
Just after 7 days
Final Diagnosis
| Serum zinc level was very low, undetectable levels. |
| He was given oral zinc supplementation in pharmacological dose. |
| Dramatic improvement with just 1 week of zinc supplementation. |
| It was a case of acrodermatitis enteropathica |
Question asked in CME INDIA group
- Was there diarrhoea? Acrodermatitis enteropathica patients’ needs lifelong zinc supplementation. Zinc gluconate/sulfate 1-3mg/kg /day
Dr. Ravishankar Dwivedi
- Yes, and that’s why I had to give therapeutic dose.
Other Inputs in the CME INDIA Group
- Treatment of acrodermatitis enteropathica requires lifelong zinc supplementation, typically 1-3 mg/kg of zinc gluconate or sulfate administered orally each day.
- Clinical improvement often occurs before significant changes in plasma zinc levels, usually within days to weeks of initiating treatment. Serum zinc levels and alkaline phosphatase values should be monitored every 3-6 months.
- Exacerbation of acrodermatitis enteropathica during pregnancy or stress may require increased therapy.
- Warm compresses to remove scale crusts, followed by the application of white petrolatum to eroded skin lesions, can enhance reepithelialization when used concurrently with zinc replacement. Regular monitoring includes periodic measurement of zinc levels, complete blood counts, erythrocyte indices, serum copper levels, and occult blood in the stool. Alkaline phosphatase levels may rise during zinc supplementation. High plasma zinc levels can inhibit copper absorption due to competitive inhibition of a common cationic transporter, potentially leading to hypocupremia, which should be monitored. Other adverse effects of zinc supplementation include gastric irritation and gastric hemorrhage.
- In cases of acquired zinc deficiency, zinc supplementation doses vary depending on the underlying cause. Patients with malabsorption may require higher doses to respond to treatment. Compresses and emollients applied to affected areas can aid re-epithelialization when used along with zinc supplementation.
CME INDIA Learning Points
Evaluate
- Acrodermatitis enteropathica typically presents during weaning in breastfed infants and earlier in formula-fed infants.
- Breastfed infants may show symptoms even before weaning due to decreased zinc secretion in breast milk caused by maternal mutations.
- Characteristic skin findings include sharply-demarcated, dry, scaly erythematous plaques, often periorificial on the face or anogenital area, with the upper lip usually spared.
- Plaques can appear psoriasiform, eczematous, vesiculobullous, pustular, or erosive with a crusted border; nail changes, brittle and lusterless hair, and diffuse alopecia in severe cases.
- Additional symptoms include angular cheilitis, delayed wound healing, and pigmentary abnormalities.
- Systemic features comprise diarrhea, irritability, lethargy, anorexia, growth retardation, anemia, amenorrhea, neuropsychiatric problems, perinatal morbidity, hypogonadism, hyposmia, hypogeusia, eye abnormalities, and immunological issues.
- Superinfection with Staphylococcus aureus and Candida albicans is reported.
- The classical triad includes alopecia, diarrhea, and a periorificial/acral cutaneous rash.
- Untreated acrodermatitis enteropathica can be fatal.
- Differential diagnoses include protein-energy malnutrition, psoriasis, seborrheic dermatitis, and glucagonoma syndrome.
- Acrodermatitis dysmetabolic describes metabolic disorders resembling AE, often due to acquired deficiencies of zinc, amino acids, or biotin.
Investigate
- Plasma zinc levels help confirm the diagnosis of acrodermatitis enteropathica, with less than 70 µg/L (fasting) or 65 µg/dL (non-fasting) considered diagnostic.
- Accurate zinc level measurement requires care to avoid contamination from tubes, catheters, needles, or rubber stoppers.
- Zinc levels can vary with time of day, stress, or inflammation; samples should be drawn in the morning using especially acid-washed glass bulbs or tubes.
- Low serum albumin can lead to low zinc levels; hence, albumin should also be measured.
- Measuring alkaline phosphatase, a zinc-dependent enzyme, may be useful.
- If diagnosis is uncertain, histopathological examination of affected skin may show psoriasiform hyperplasia with necrolysis, cytoplasmic pallor, confluent parakeratosis, spongiosis, and focal dyskeratosis, although these findings are not diagnostic.
Treat
- Management of acrodermatitis enteropathica involves enteral or parenteral zinc supplementation, typically requiring lifelong supplementation with 3 mg/kg/day of elemental zinc.
- Zinc sulfate is the preferred oral formulation (4 mg of zinc sulfate contains about 1 mg of elemental zinc), and zinc chloride is preferred for parenteral supplementation.
- Clinical response to treatment is often dramatic, with reduced irritability and improved skin lesions noted within a few days of initiating treatment.
- Regular monitoring during therapy includes periodic measurement of zinc levels, complete blood counts, erythrocyte indices, serum copper levels, and occult blood in the stool.
- Alkaline phosphatase levels may rise during zinc supplementation.
- High plasma zinc levels can inhibit copper absorption, leading to hypocupremia, which should be monitored.
- Other adverse effects of zinc supplementation include gastric irritation and gastric hemorrhage.
- In cases of acquired zinc deficiency, zinc supplementation doses vary depending on the underlying cause, with higher doses needed for patients with malabsorption.
- Compresses and emollients applied to affected areas may aid re-epithelialization when used alongside zinc supplementation.
CME INDIA Tail-Piece
- Another 9 months old child with Acrodermatitis enteropathica
- Acrodermatitis enteropathica (AE) is an inherited zinc deficiency caused by a defect in zinc absorption. Zinc is a crucial micronutrient, part of over 200 metalloenzymes, and is essential for various metabolic and biochemical pathways.
- AE results from mutations in the zinc transporter gene SLC39A4 (solute carrier family 39 member A4), leading to impaired enteral zinc absorption.
- AE was first described by Brandt in 1936 and later recognized as a distinct disease by Danbolt and Closs.
- Zinc deficiency can also be acquired due to malabsorption syndromes, liver or kidney disease, dietary habits, and iatrogenic causes, presenting with similar clinical features to AE.
Further Reading:
- Ciampo IRLD, Sawamura R, Ciampo LAD, Fernandes MIM. ACRODERMATITIS ENTEROPATHICA: CLINICAL MANIFESTATIONS AND PEDIATRIC DIAGNOSIS. Rev Paul Pediatr. 2018 Apr-Jun;36(2):238-241.
- Jagadeesan S, Kaliyadan F. Acrodermatitis Enteropathica. 2023 Apr 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 28722865.
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Excellent Platform for daily learning and interactions
Find the plateform refreshing and improving clinical sense.
Excellent sir.
Hypo cupremia can produce sub acute combined degeneration like picture as it affects spinal cord. So oral zinc should be taken 2 hours after food once in a day. Zinc and copper have same receptors in the stomach.