
CME INDIA Presentation by Dr. Raman Puri, Chairman, Senior Consultant Cardiologist, Cardiac Care Centre, New Delhi.
(Co-authors : Vimal Mehta, Manish Bansal, P Barton Duell, S S Iyengar, Sadanand Shetty, Ian Graham, J C Mohan, Upendra Kaul, Dayasagar Rao, Rajeev Agarwala, Gurpreet Singh Wander, Prakash Hazra, Soumitra Kumar, S K Wangnoo, Abdul Hamid Zargar, Banshi Saboo, Jamal Yusuf, Vinod M Vijan, Prem Aggarwal, Sarat Chandra, Ravi R Kasliwal, P C Manoria, M U Rabbani, Milan C Chag, D Prabhakar, Aziz Khan, Neil Bordoloi, Saravanan Palanippan, Kunal Mahajan, Akshay Pradhan, Dharmender Jain, A Murugnathan, Pradeep Kumar Dabla, Nagaraj Desai, Mangesh H Tiwaskar, Devaki R Nair, Charanjeet Singh, Jayant Panda, Vitull Gupta, Prashant Sahoo, Nathan D Wong.)
To address India’s ASCVD epidemic, more intensive LDL-C and non-HDL-C lowering is required
- The incidence of adverse cardiovascular (CV) events has decreased in Western countries, primarily due to aggressive risk factor control and effective dyslipidemia management. In the U.S., mean LDL-C levels dropped from 126.2 mg/dL in 1999–2000 to 112.8 mg/dL in 2015–16, leading to a reduction in CV and ischemic heart disease (IHD) mortality by 60%. In contrast, India experienced a 31% increase in CV mortality among men and a 13% increase among women between 1990–2015. This disparity is attributed to inadequate control of risk factors, especially dyslipidemia, which plays a crucial role in atherosclerosis development.
- Dyslipidemia is a significant driver of CV risk in India, with the INTERHEART study showing that it accounts for nearly 50% of the population-attributable risk for myocardial infarction. The ICMR-INDIAB study revealed that 79% of Indians have at least one dyslipidemic feature, with low HDL-C present in 72.3% and hypertriglyceridemia in 29.5% of the population. Although only 11.8% have high LDL-C, the presence of small, dense LDL particles and elevated Apo B levels indicate high atherogenicity.
- To address India’s ASCVD epidemic, more intensive LDL-C and non-HDL-C lowering is required, targeting not just LDL-C levels but also reducing LDL particle numbers and Apo B, which are stronger predictors of atherosclerosis risk.
LAI Points towards Very Urgent Need
- The Lipid Association of India (LAI) recognized the need for more aggressive dyslipidemia management in India, leading to the formulation of tailored recommendations with lower LDL-C and non-HDL-C targets for the Indian population. After extensive discussions with experts across the country, the LAI published its first Expert Consensus Statement in 2016, recommending an LDL-C target of <50 mg/dL for very high-risk patients, including those with ASCVD and diabetes with additional risk factors. This target was lower than those in Western guidelines, reflecting the earlier onset and more aggressive nature of ASCVD in Indian populations.
- Subsequent research, including findings from the IMPROVE-IT and ODYSSEY OUTCOMES trials, demonstrated the need for even more stringent LDL-C targets. Despite achieving LDL-C levels of around 53 mg/dL in these studies, many high-risk patients continued to experience recurrent CV events. This prompted the LAI to update its recommendations in 2020, introducing an extreme risk group (ERG) for patients with ASCVD and multiple high-risk features, recommending LDL-C targets as low as ≤30 mg/dL, with an optional goal of ≤30 mg/dL in some cases.
- The latest LAI guidelines have incorporated further evidence from trials like the FOURIER study, which demonstrated additional benefits with LDL-C levels as low as 30 mg/dL. The most recent update also introduces a new extreme risk category C for patients with recurrent events despite achieving LDL-C levels around 30 mg/dL, recommending LDL-C lowering to 10–15 mg/dL for this group.
Rationale for Lower Low-Density Lipoprotein Cholesterol (LDL-C) Targets for Indian Subjects
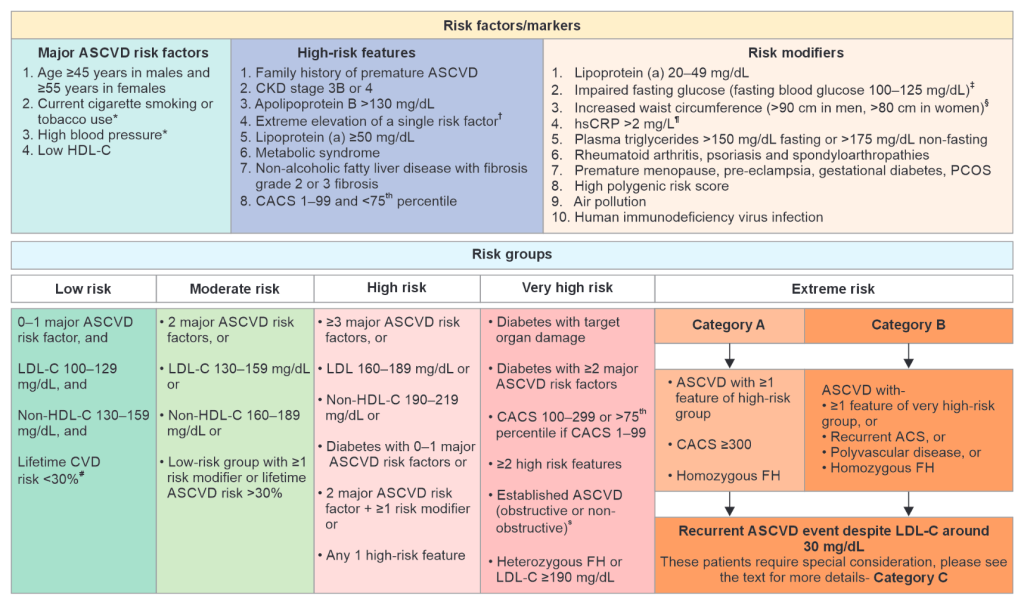
Updated 2023 risk stratification approach recommended by the Lipid Association of India (Reproduced with permission from Puri et al.)
- The Lipid Association of India (LAI) recommended lower LDL-C targets for Indian subjects (<50 mg/dL and ≤30 mg/dL) compared to European guidelines (≤55 mg/dL and 40 mg/dL). This decision is based on the unique characteristics of atherosclerotic cardiovascular disease (ASCVD) in Indians. Indians experience coronary artery disease (CAD) at a younger age than Western populations, with higher rates of premature heart attacks and deaths. Despite having lower baseline LDL-C levels than Western populations, Indians face a higher risk of premature CAD, necessitating more aggressive LDL-C lowering.
- In addition to high LDL-C levels, Indians have elevated triglycerides, higher non-HDL-C, and small, dense LDL particles, all of which contribute to increased ASCVD risk. Elevated Apo B levels and lipoprotein(a) [Lp(a)], both of which are more prevalent in Indians, further accelerate atherosclerosis. These factors, along with small coronary arteries, make aggressive lipid-lowering strategies crucial for reducing cardiovascular events.
- Given these risk factors, the LAI recommends lower LDL-C, non-HDL-C, and Apo B goals to improve cardiovascular outcomes in Indians. The American College of Cardiology/American Heart Association has also recognized South Asian ancestry as a risk enhancer for ASCVD, aligning with the LAI’s lower LDL-C targets. Moreover, studies have shown that achieving ultra-low LDL-C levels is safe and significantly reduces cardiovascular events. Therefore, the LAI’s recommendations are vital for addressing the specific cardiovascular risks faced by Indian populations.
Treatment targets for lipid lowering therapy for various ASCVD risk groups
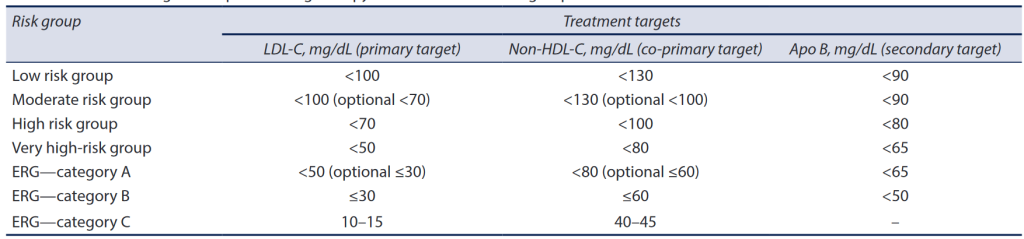
(Reproduced with permission from Puri et al.)
LAI Take home Message
- Western LDL-C targets may not be appropriate for the Indian population, as they could lead to increased cardiovascular (CV) risk. Indians have a unique lipid profile, with lower baseline LDL-C levels, high triglycerides, low HDL-C, dysfunctional HDL particles, and elevated Apo B and lipoprotein(a) [Lp(a)] levels, all of which contribute to a higher risk of atherosclerotic cardiovascular disease (ASCVD).
- Due to the earlier onset and aggressive nature of coronary artery disease (CAD) in Indians, along with these risk factors, more aggressive LDL-C lowering is necessary.
- The Lipid Association of India (LAI) recommends lower LDL-C targets (<50 mg/dL and ≤30 mg/dL for high- and extreme-risk groups) to effectively reduce ASCVD in India. Implementing these guidelines will help manage dyslipidemia and lower the risk of CV events in Indian patients.
CME INDIA Learning Points
| 1. Western CV Event Reduction Success: Aggressive risk factor control, particularly dyslipidemia management, has contributed to a decline in cardiovascular (CV) events in Western countries. The American and European dyslipidemia treatment guidelines have significantly reduced atherosclerotic cardiovascular disease (ASCVD) in these populations. |
| 2. Inappropriateness of Direct Guideline Extrapolation: Directly applying Western dyslipidemia guidelines to Indian patients is not suitable due to different risk profiles and patterns of dyslipidemia, requiring unique treatment approaches for the Indian population. |
| 3. Dyslipidemia and CV Risk in India: India faces poor control of dyslipidemia and risk factors, leading to an increase in CV and coronary artery disease (CAD) mortality. Dyslipidemia contributes to about 50% of the population-attributable risk for myocardial infarction in India. |
| 4. Unique Indian Dyslipidemia Patterns: Indian populations exhibit a distinct pattern of dyslipidemia, characterized by lower LDL-C, higher triglycerides, and lower HDL-C levels compared to Western populations. This necessitates unique lipid management strategies and lower LDL-C targets for Indians. |
| 5. LAI’s LDL-C Recommendations for Indians: The Lipid Association of India (LAI) recommends lower LDL-C targets for Indians—<50 mg/dL for those with ASCVD or diabetes with additional risk factors, and ≤30 mg/dL for individuals at extremely high risk—due to the earlier onset and more aggressive nature of CAD in Indians. |
| 6. Hypertriglyceridemia and Atherogenic Lipoproteins: Approximately 30% of Indians have hypertriglyceridemia, increasing ASCVD risk. Elevated atherogenic triglyceride-rich lipoproteins, small dense LDL particles, and apolipoprotein B (Apo B) levels contribute to a higher burden of circulating atherogenic particles in Indians. |
| 7. Impact of Low HDL-C and Elevated Lp(a): Many Indians have low HDL-C levels, which are often dysfunctional, and elevated lipoprotein(a) [Lp(a)] levels, further increasing atherogenicity and premature CAD risk. |
| 8. Importance of Lower Targets for Indian Patients: Given the more aggressive nature of dyslipidemia and ASCVD in Indian populations, lower LDL-C, non-HDL-C, and Apo B goals than those in Western guidelines are required to effectively manage ASCVD risk in Indians. |
| 9. South Asian Ancestry as a Risk Enhancer: American lipid management guidelines identify South Asian ancestry, including Indians, as a risk enhancer, underscoring the need for more aggressive LDL-C lowering in this group. |
| 10. Potential Harm from Western LDL-C Targets in Indians: Western LDL-C targets may be too high for Indian populations, leading to higher residual ASCVD risk and preventable CV events, which could be mitigated with lower LDL-C targets. |
| 11. Incremental Benefits of LDL-C Reduction: Mendelian randomization studies suggest that lowering LDL-C by 5–10 mg/dL reduces CV risk by 8–18%, supporting the LAI’s recommendation for lower LDL-C targets to achieve these benefits. |
| 12. What to Infer: Indian populations require more aggressive LDL-C and non-HDL-C lowering, as recommended by the LAI, to combat the heightened ASCVD risk and stem the ongoing epidemic of cardiovascular diseases in India. |
Further Readings:
- Puri R, Mehta V,Bansal M, et al. Does Adopting Western Low-density Lipoprotein Cholesterol Targets ExposeIndians to a Higher Risk of Cardiovascular Events?Expert Opinion From the Lipid Association ofIndia. J Assoc Physicians India 2024;72(10):71–76.
- Yusuf S, Hawken S, Ounpuu S, et al. Ef fect ofpotentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case control study. Lancet 2004;364:937–952.
- Joshi SR, Anjana RM, Deepa M, et al. Prevalence of dyslipidemia in urban and rural India: The ICMR–INDIAB Study. PLoS ONE 2014;9:e96808.
- Puri R, Mehta V, Iyengar SS, et al. Lipid Association of India expert consensus statement on management of dyslipidemia in Indians 2020: part III. J Assoc Phys India 2020;68(11):8–58.
- Puri R, Mehta V, Duell PB, et al. Proposed low-density lipoprotein cholesterol goals for secondary prevention and familial hypercholesterolemia in India with focus on PCSK9 inhibitor monoclonal antibodies: expert consensus statement from Lipid Association of India. J Clin Lipidol 2020;14:e1–e13
- Puri R, Bansal M, Mehta V, et al. Lipid Association of India 2023 update on cardiovascular risk assessment and lipid management in Indian patients: consensus statement IV. J Clin Lipidol 2024;18(3):e351–e373
- Mehta V, Iyengar SS, Yusuf J, et al. Fighting the atherosclerotic cardiovascular disease epidemic: declaring war on lipids by Lipid Association of India.J Assoc Physicians India 2020;68(11):6–7
- Berry P, Amarchand R, Ramakrishnan L, et al.Establishing apolipoprotein-B and non-high-density-lipoprotein-C goals in Indian population: a cross-sectional study. Indian Heart J 2024:76(3):154–158.
- Anand SS, Enas EA , Pogue J, et al. Elevated lipoprotein(a) levels in South Asians in North America.Metabolism 1998;47(2):182–184
- Kalra D, Vijayaraghavan K, Sikand G, et al. Prevention of atherosclerotic cardiovascular disease in South Asians in the US: a clinical perspective from the National Lipid Association. J Clin Lipidol 2021;15:402–422.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
I wanted some clarification on these issues.
1. It takes 20 people to give a statin therapy to get one meaningful result.
2. The CV mortality in the us has come down not only by LDL, it is a contributing factor but not an absolute one . Well controlled hypertension, awareness and smoking cessation is also a reason.
3. I agree on the CV burden of our nation and the early onset of these conditions, but can it be absolutely blamed on LDL and appoB lip a , without factoring insulin resistance, hypertension , smoking and very poor physical activities.
4. Will pushing LDL so low will not have a J shaped response in having unwanted repercussions..
I look forward for your valuable feedback,
This is a very valid question. In order for atherosclerosis to initiate and progress, cholesterol must be present, whether it comes from LDL, LPA, IDL, or tryglyceride-rich VLDL remanent lipoprotein particles. Smoking and HT can only cause endothelial dysfunction, making cholesterol-containing lipoproteins and monocytes easier to enter subintimal spaces, resulting in foam cells. According to strong scientific evidence, only LDL-C has a causal relationship with Atherosclerotic Cardiovascular Disease (ASCVD). IR leads to atherogenic dyslipidemia, which causes atherosclerosis. Atherogenic small dense LDL-C particles are associated with IR. There is no threshold below which CV event reduction is not observed in LDL-C, as seen in the Fourier and Odessey trials. To reduce CV events, you should not only lower LDL-C targets as advised by the ASCVD risk group, but also control all modifiable risk factors and residual risk. You should remember that the targets for each ASCVD risk group are based on strong scientific evidence. This is whether it is less than 50 mg/dl or less than 30 mg/dl. Secondary causes of dyslipidemia should also be treated. It goes without saying that modifying your lifestyle is essential for managing dyslipidemia and reducing cardiovascular disease risks.
To date, only LDL-C has been shown to be causally related to ASCVD. The results of the Horizan Trial will provide information about the association between LPA and ASCVD. Until now, only epidemiological studies, meta-analyses, and genome-wide association studies have linked elevated LPA to MI, stroke, PAD, heart failure, and death. LPA is undoubtedly pro-atherosclerotic, prothrombotic, and pro-inflammatory. According to LAI recommendations, everyone should be screened for lipid profile including LPA at age 20 or earlier, at age 2, if a family has a history of premature CAD or a family history of hypercholesterolemia or elevated LPa levels. In case LPa exceeds 50mg/dl without any ASCVD risk factors, stratify the patient into a high risk group (HRG) and decrease LDL-C to less than 70mg/dl, and if it is between 20 and 49mg/dl, it becomes a non-conventional risk factor and the low risk group (LRG) is reclassified into a moderate risk group (MRG) and MRG is reclassified as a HRG. Achieve LDL-C goals based on ASCVD risk group.
Very clearly explained. I have a question: LP(a) is, in a recent review, said to be six times more atherogenic than LDLc, although the later is more abundant in blood. How to tackle LPa in Indian context?