

CME INDIA Presentation by Dr. Parimal Swamy, MD, Diploma in Preventive Health Care (Apollo Hospital, Hyderabad), Certificate of Excellence in Diabetes Care (NIMS, Hyderabad), W.H.O. Accredited Diploma in Diabetes Management, Certificate of Diabetes Specialization (Germany), Certified Cardiac Rehab Facilitator (Univ. of York, U.K.) Consultant Physician JH & RC, Professor (Medicine) HIDS, Director Apollo Asthma & Diabetes Care Centre, Jabalpur.
Are we ready to embrace the change, and what might it mean for the future of diabetes management?
- In the evolving landscape of medical science, diabetes remains a formidable challenge, affecting millions worldwide with its multifaceted complexities.
- As we stand at a pivotal moment, “Navigating the Crossroads: Rethinking the Classification and Diagnosis of Diabetes” delves into the urgent need to reassess our understanding of this metabolic disorder.
- Traditional classifications have served us well, yet the emergence of new research, technologies, and patient data compels us to question if these frameworks still capture the full spectrum of this condition.
- This introduction to a new era in diabetes care explores how advancements in genetics, precision medicine, and personalized health data are pushing us towards a more nuanced, effective diagnostic and classification system. Are we ready to embrace this change, and what might it mean for the future of diabetes management?
Diabetes as it is today
- Type 1 diabetes (due to autoimmune β-cell destruction, usually leading to absolute insulin deficiency, including latent autoimmune diabetes in adults).
- Type 2 diabetes (due to a non-autoimmune progressive loss of adequate β-cell insulin secretion, frequently on the background of insulin resistance and metabolic syndrome).
- Specific types of diabetes due to other causes, e.g., monogenic diabetes syndromes (such as neonatal diabetes and maturity-onset diabetes of the young), diseases of the exocrine pancreas (such as cystic fibrosis and pancreatitis), and drug- or chemical-induced diabetes (such as with glucocorticoid use, in the treatment of people with HIV, or after organ transplantation).
- Gestational diabetes mellitus (diabetes diagnosed in the second or third trimester of pregnancy that was not clearly overt diabetes prior to gestation or other types of diabetes occurring throughout pregnancy, such as type 1 diabetes).
Most Widely Followed Criteria

Courtesy: ADA 2025
‘Subtle Changes’ to the ADA Standards of Care in Diabetes – Diagnosis and Classification of Diabetes.”
- Recommendation 2.5 says to classify people with hyperglycemia into appropriate diagnostic categories to aid in personalized management.
- “Diabetes is conveniently classified into several clinical categories, although these are being reconsidered based on genetic, metabolomic, and other characteristics and pathophysiology.“
- It means is, first, let’s figure out whether this patient does or does not have diabetes and then we’ll try to classify it, but it might not fit into those simple categories that we all were trained on. It may not be classic type 1, classic type 2, classic other, or gestational diabetes (What is this? We really need to think that way.)-Anne L. Peters, MD: commentary on ADA 2024 Guidelines; Medscape, January 2024.
Understanding Endotypes of Type 1 Diabetes

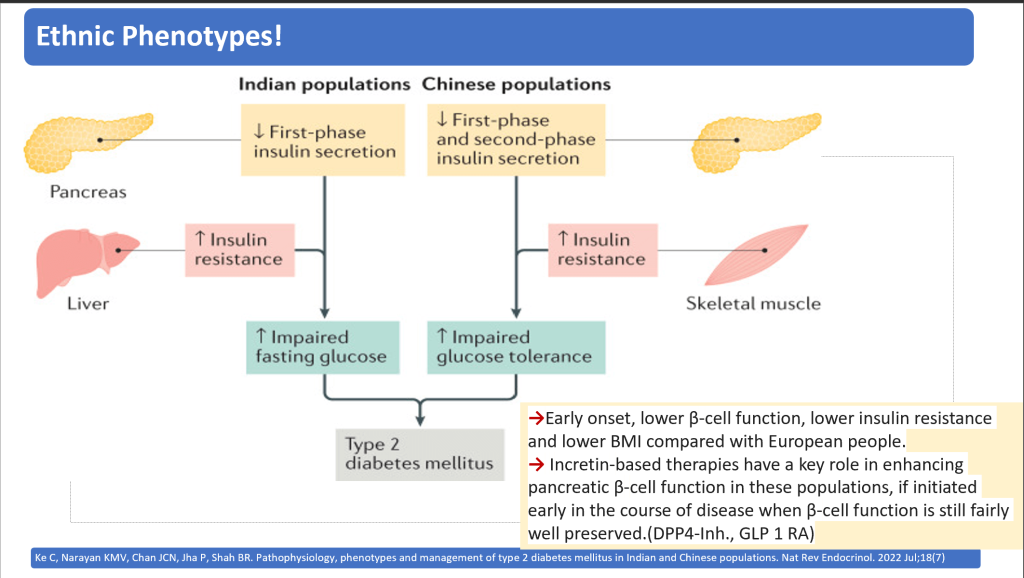
Ethnic Phenotypes differ
Genetics is in Focus

Problem with Traditional Classification

A: The traditional classification of diabetes where T1D and T2D are viewed as distinct subgroups but with an overlap including intermediate diabetes types such as LADA. Monogenic and secondary diabetes are rare, etiologically distinct subtypes that are not included in the novel subclassification.
B: The palette model where the many molecular pathways involved in diabetes pathogenesis are represented as colors and each individual with T2D is represented by the mixed colors of all the pathways affected in that individual
C: The ANDIS model, where colors instead represent clinical parameters, reflecting the underlying mechanisms, that are easy to measure in the clinic. With this approach, individuals are grouped based on their main color into subtypes with different clinical characteristics.

Courtesy: Emma Ahlqvist, Rashmi B. Prasad, Leif Groop; Subtypes of Type 2 Diabetes Determined From Clinical Parameters. Diabetes 1 October 2020; 69 (10): 2086–2093
The current classification of diabetes mellitus complicates diagnosis and treatment
- The current classification of diabetes mellitus (DM) complicates diagnosis and treatment due to its unclear definitions of type 1 DM, type 2 DM, and LADA.
- It also fails to integrate new disease insights. It was suggested in 2016 by Schwartz SS et al that a β-cell-centric classification, focusing on the abnormal pancreatic β-cell as the common root of all DM.
- The new model considers how genetically predisposed β-cells interact with factors like insulin resistance, environmental influences, and immune issues, leading to various forms of hyperglycemia through 11 pathways.
- This new approach allows for personalized treatments targeting specific hyperglycemia mechanisms, avoiding hypoglycemia, weight gain, and additional β-cell stress. We urge a review of the current DM classification to adopt this more effective system.
| SAID (Autoimmune) requires early introduction of insulin supplementation, |
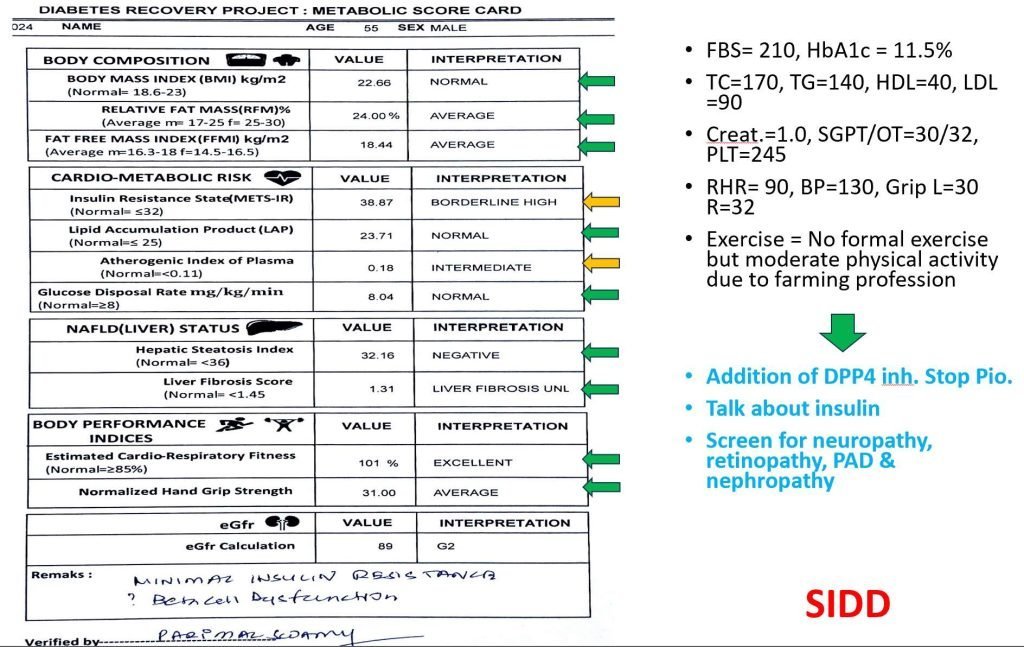
| SIDD (Insulin Deficiency)may also benefit from a dipeptidyl peptidase 4 inhibitor (DPP4i) or, when cost is a major issue, a sulfonylurea. (!GLP-1RA early). |
| SIRD(Insulin Resistance) and MOD(↑ Fat Mass) would benefit from medication that induces weight loss (SGLT2i, GLP-1RA, dual agonist) or also addresses risk of CVD or nephropathy (SGLT2i, GLP-1RA). |
| Providing that safety and efficacy have been established, new insulin sensitizers (e.g. peroxisome proliferator activator receptor agonists) or anti-inflammatory drugs could also improve targeted treatment of SIRD(Insulin Resistance). |
| MARD(Aging) should receive treatments avoiding weight loss and sarcopenia (e.g. protein-balanced diets and moderate resistance training). |
Functional Classification of Diabetes!
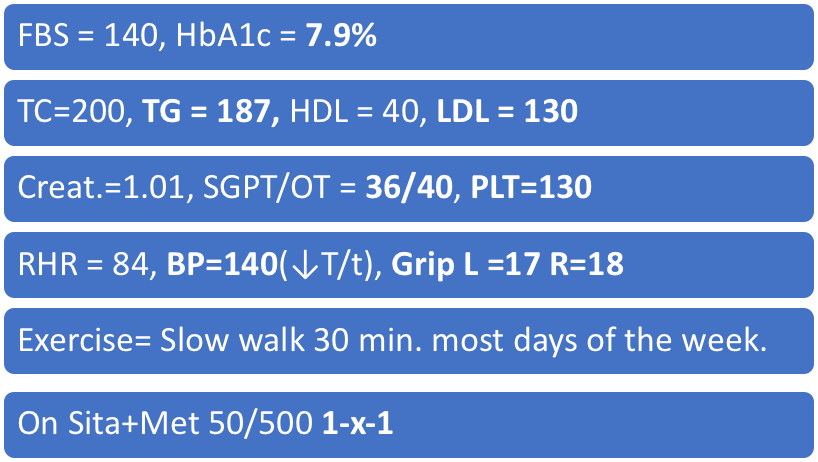
Case 1
40 YRS. Female; duration = 5 yrs., urban, housewife
wt.= 60 kg, ht.= 150 cm, waist = 80 cm, BMI = 26.67, Hypn.(↓T/t), family history of DM +
Modifications Matter

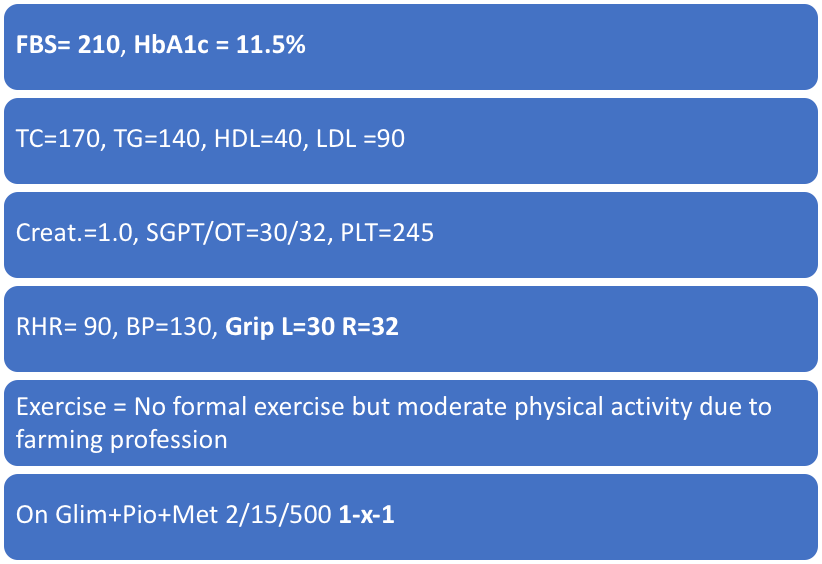
Case 2
55 Yrs. Male; duration = 4 years., rural, farmer
wt.= 58 kg, ht.=160 cm, waist=80 cm, BMI=22.66, tobacco +, no family history
And modification matters
Take Home Points

CME INDIA Tail Piece
- Staging schema for early diagnosis of prediabetes by Bergman, Michael et al. has been introduced. (The Lancet Diabetes & Endocrinology, Volume 12, Issue 12, 873 – 876)
- It is a novel staging schema aimed at the early detection of prediabetes and type 2 diabetes through the use of 1-hour plasma glucose (1hPG) levels.
- This approach was recently endorsed by the International Diabetes Federation in a Position Statement, emphasizing its utility in diagnosing hyperglycemia earlier in its progression, thereby potentially improving long-term health outcomes. Is it rational to do so?
- The conventional metrics for diabetes screening—fasting plasma glucose (FPG), 2-hour plasma glucose (2hPG), and hemoglobin A1c (HbA1c)—are well-established but may miss individuals at high risk who could benefit from early intervention.
- Recent evidence supports the use of 1hPG as an additional screening tool, particularly because individuals with a 1hPG of ≥155 mg/dL (8.6 mmol/L) but normal glucose tolerance (NGT) are shown to be at a heightened risk for developing type 2 diabetes, alongside increased risks for cardiovascular complications and premature mortality.
- Staging Schema and Clinical Implications:
- Prediabetes: A 1hPG level of ≥155 mg/dL (8.6 mmol/L) in individuals with NGT indicates a significant risk for progression to type 2 diabetes. This stage calls for immediate lifestyle interventions, which have proven effective in delaying or preventing the onset of diabetes.
- Type 2 Diabetes: A 1hPG level of ≥209 mg/dL (11.6 mmol/L) during a 75 g oral glucose tolerance test (OGTT) should be considered indicative of type 2 diabetes. This diagnosis requires confirmation through a repeat test.
- Implementation in Clinical Practice:
- The inclusion of 1hPG in routine screening could enhance our ability to intervene at an earlier stage of the disease. This is crucial because early intervention, particularly through lifestyle changes, can significantly alter the progression of diabetes and its complications. Therefore, in Indians ,CME INDIA is in favor that the 1hPG measurement be integrated into the standard OGTT protocol, alongside existing measures of FPG, 2hPG, and HbA1c.
- Is it cost effective? – Screening for prediabetes using 1hPG has been demonstrated to be both feasible and cost-effective, offering a practical approach to identifying at-risk individuals before the onset of full-blown diabetes. This could lead to substantial savings in healthcare costs by preventing or delaying the need for more intensive treatments and managing complications associated with advanced diabetes.
- What We Expect? – By adopting this staging schema, clinicians can better identify and manage individuals at risk for or in the early stages of diabetes. This proactive approach not only aligns with the latest evidence but also supports the broader goal of reducing the global burden of type 2 diabetes through early detection and intervention.
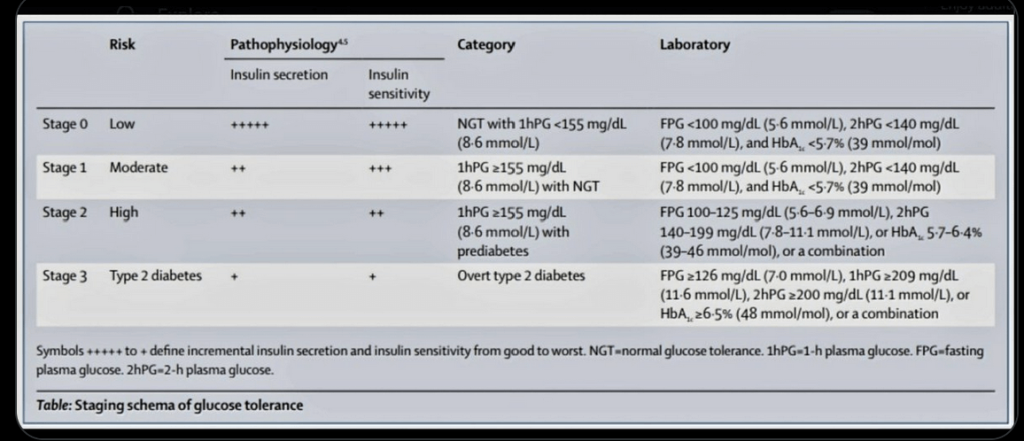
Courtsey: Bergman, Michael et al.Staging schema for early diagnosis of prediabetesThe Lancet Diabetes & Endocrinology,2024
References:
- Bergman, Michael et al.Staging schema for early diagnosis of prediabetesThe Lancet Diabetes & Endocrinology,2024; Volume 12, Issue 12, 873 – 876
- Bergman M, Manco M, Satman I, Chan J, Schmidt MI, Sesti G, Vanessa Fiorentino T, Abdul-Ghani M, Jagannathan R, Kumar Thyparambil Aravindakshan P, Gabriel R, Mohan V, Buysschaert M, Bennakhi A, Pascal Kengne A, Dorcely B, Nilsson PM, Tuomi T, Battelino T, Hussain A, Ceriello A, Tuomilehto J. International Diabetes Federation Position Statement on the 1-hour post-load plasma glucose for the diagnosis of intermediate hyperglycaemia and type 2 diabetes. Diabetes Res Clin Pract. 2024 Mar;209:111589. doi: 10.1016/j.diabres.2024.111589. Epub 2024 Mar 7. PMID: 38458916.
- Ha J, Chung ST, Bogardus C, Jagannathan R, Bergman M, Sherman AS. One-hour glucose is an earlier marker of dysglycemia than two-hour glucose. Diabetes Research and Clinical Practice. 2023 Sep 1;203:110839.
- Cefalo CM, Riccio A, Fiorentino TV, Succurro E, Mannino GC, Perticone M, Sciacqua A, Andreozzi F, Sesti G. Pathophysiological characteristics of subjects with intermediate hyperglycemia and type 2 diabetes identified by 1-hour plasma glucose during an oral glucose tolerance test. Diabetes Research and Clinical Practice. 2024 Nov 1;217:111856.
- Bergman M, Buysschaert M, Ceriello A, Hussain A, Mohan V, Sesti G, Tuomilehto J. Current diagnostic criteria identify risk for type 2 diabetes too late. The Lancet Diabetes & Endocrinology. 2023 Apr 1;11(4):224-6.
- American Diabetes Association Professional Practice Committee; 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes—2025. Diabetes Care 1 January 2025; 48 (Supplement_1): S27–S49. https://doi.org/10.2337/dc25-S002
- Ke C, Narayan KMV, Chan JCN, Jha P, Shah BR. Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations. Nat Rev Endocrinol. 2022 Jul;18(7)
- Schwartz SS, Epstein S, Corkey BE, Grant SF, Gavin JR 3rd, Aguilar RB. The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema. Diabetes Care. 2016 Feb;39(2):179-86.
- Herder, C., Roden, M. A novel diabetes typology: towards precision diabetology from pathogenesis to treatment. Diabetologia 65, 1770–1781 (2022).
- 10.Schwartz SS, Epstein S, Corkey BE, Grant SF, Gavin JR 3rd, Aguilar RB. The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell-Centric Classification Schema. Diabetes Care. 2016 Feb;39(2):179-86.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
I would like to say, about more than 45 years ago Prof Dr Viswanathan father of Diabetes Chennai Tamilnadu , Mohan’s diabetic centre had studied extensively on his patients and wrote an article and his findings that 1 hrs glucose values of more than 155 he/ she is bound to get Diabetes following few years. In prediabetes the silent CV events are more. I am doing this test for screning my suspected patient’s in my practice for nearly 50 years.
I am happy now it is been acknowledged. Thank you for this article.
I want this ppt
good ppt intrested in getting it for academic purpose