

CME INDIA Presentation by Dr. Saptarshi Bhattacharya, MD, DM, Senior Consultant, Indraprastha Apollo Hospitals, New Delhi.
(Based on a presentation at Hormone India Conference,11th-12th January, 2025, Bhopal. This presentation is inspired by Dr. Banshi Saboo, Ahmedabad).
Let us see this case
- 33-year lady
- History of left-sided renal colic 2 years back
- USG-KUB – 5 mm ureteral stone (no other structural anomaly)
- Stone passed spontaneously
- Current problem – on routine USG – Right-sided 8 mm renal calculi
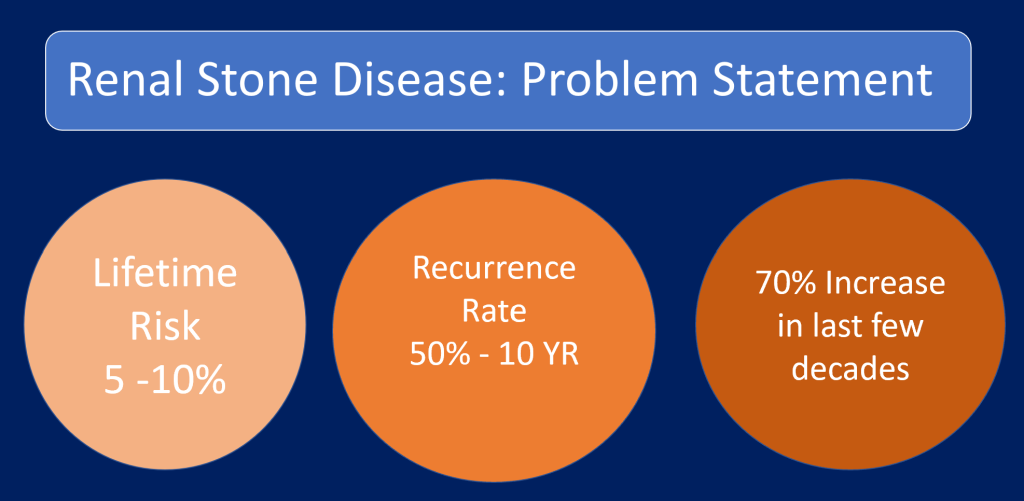
How common is renal stone disease?
Approach

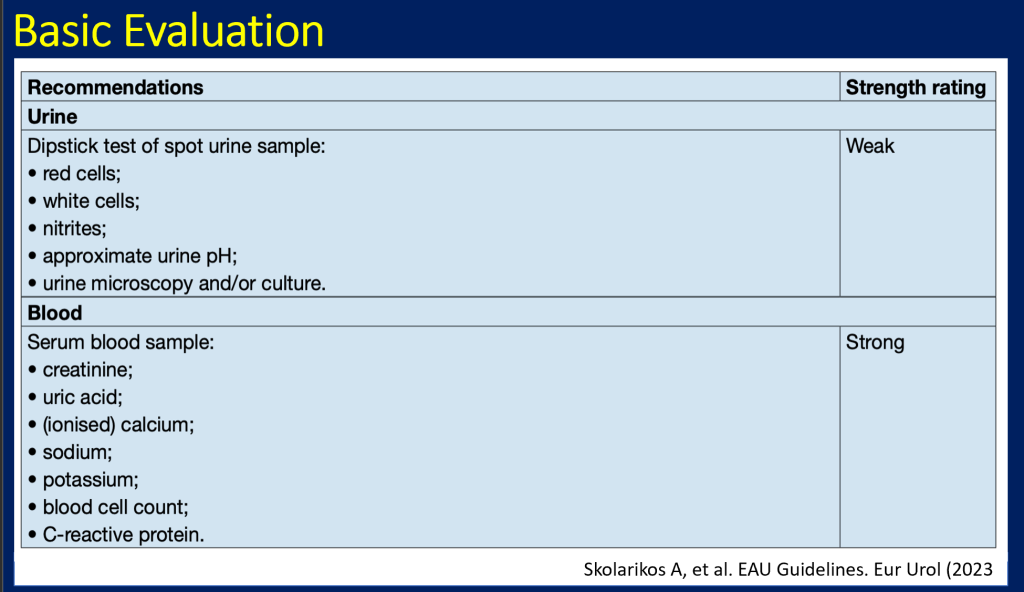
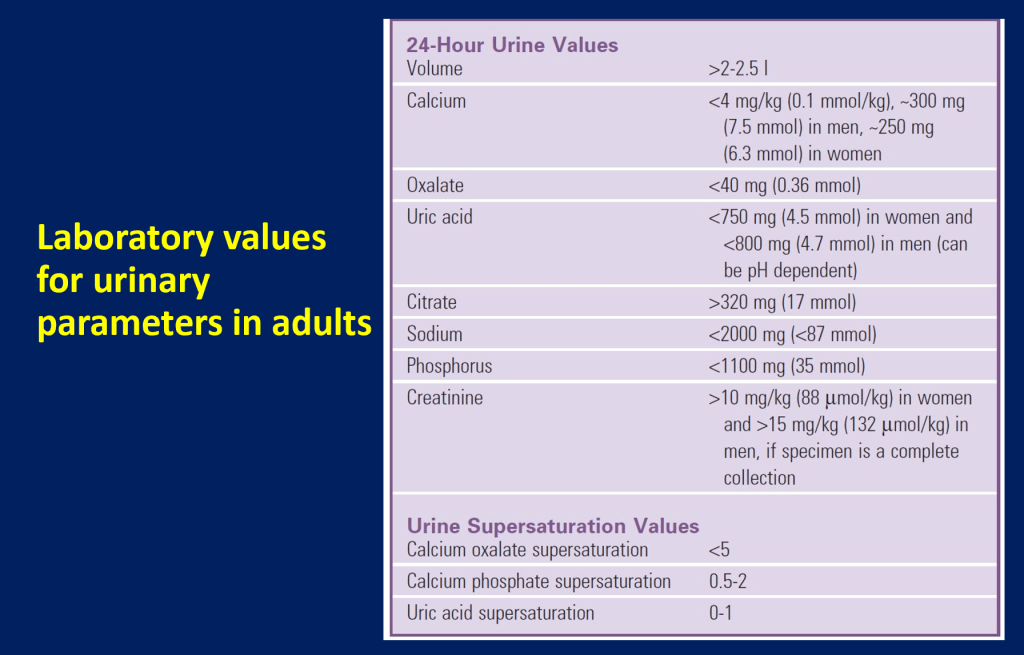
Laboratory Evaluation

Targeted Approach: Complete Evaluation in High-Risk Patients
- More than one kidney stone
- Family history of stones
- Chronic diarrheal states and/or malabsorption, pathologic fractures, osteoporosis, UTI, diabetes, and/or gout
Medication that may put them at higher risk (eg, topiramate, acetazolamide)
- Stones composed of cystine, uric acid, or calcium phosphate
- Patients with dietary habits associated with higher risk of stone formation
Complete Evaluation
- Both blood and urine testing
- Including at least two 24-hour urine collections at baseline
- Usual diet
- Free of stone for 20 days
- 1-2 months after acute stone episode
Case 1: Continued
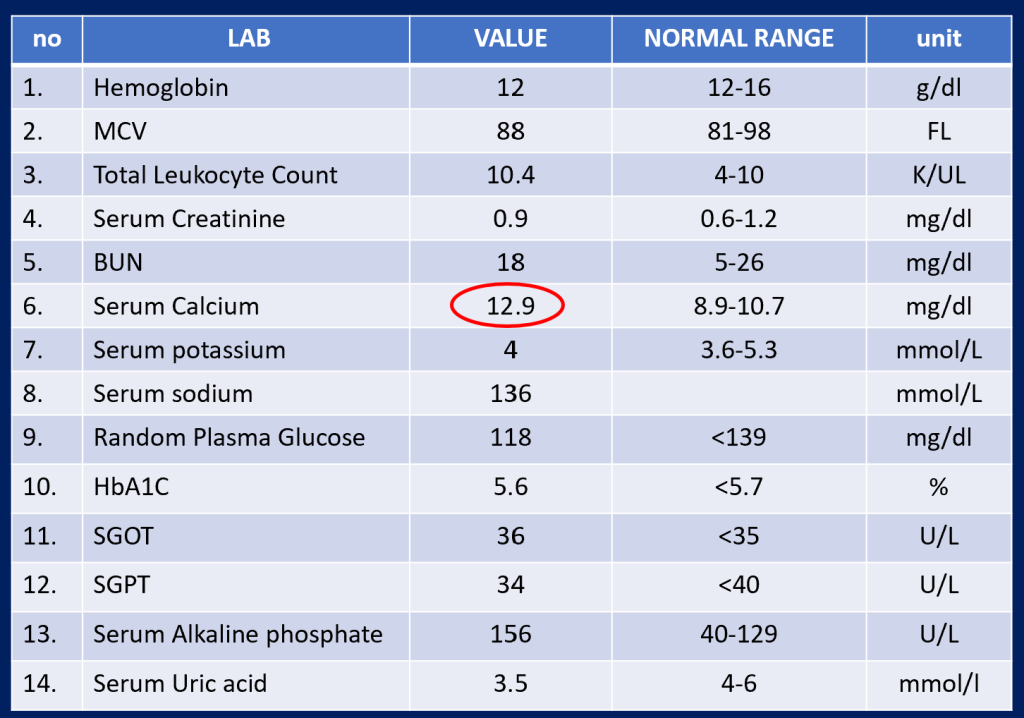
Further Labs
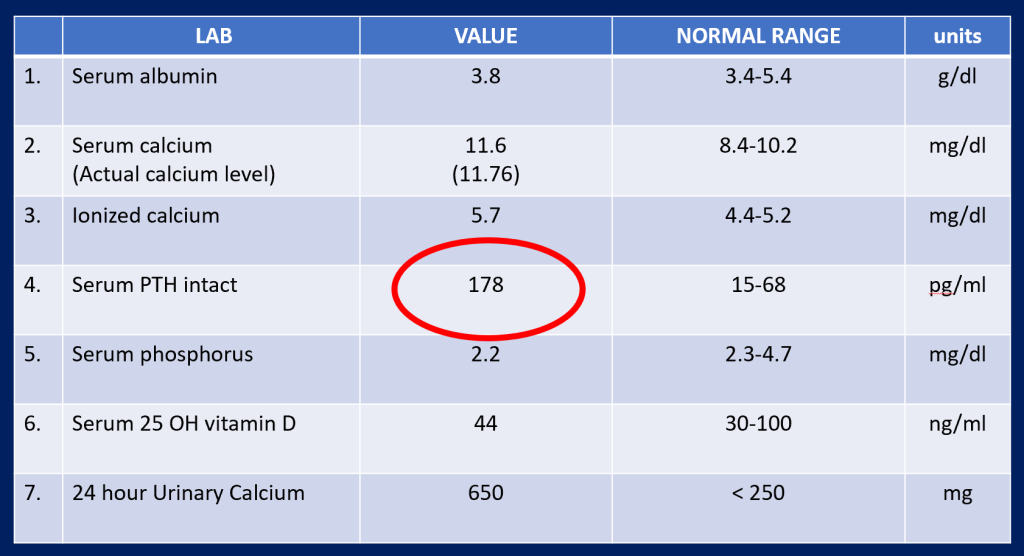
Case 1: Summary
- 33/F, Recurrent renal calculi, high calcium and PTH, High Urinary Calcium/creatinine ratio: Primary hyperparathyroidism
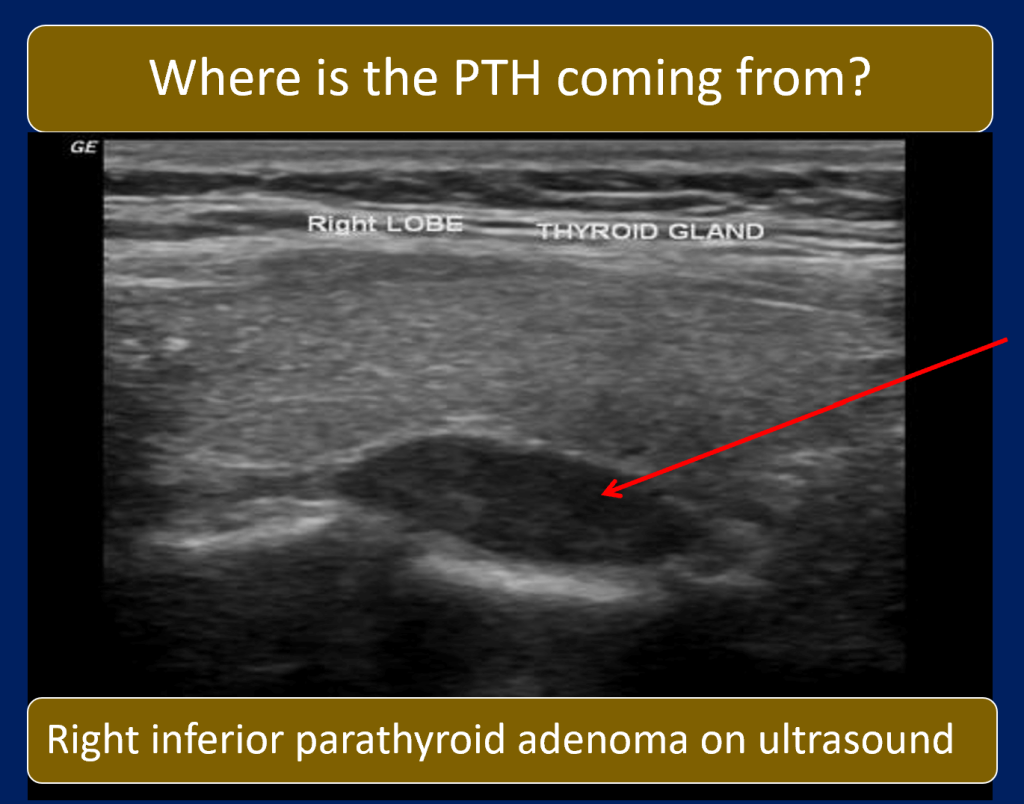
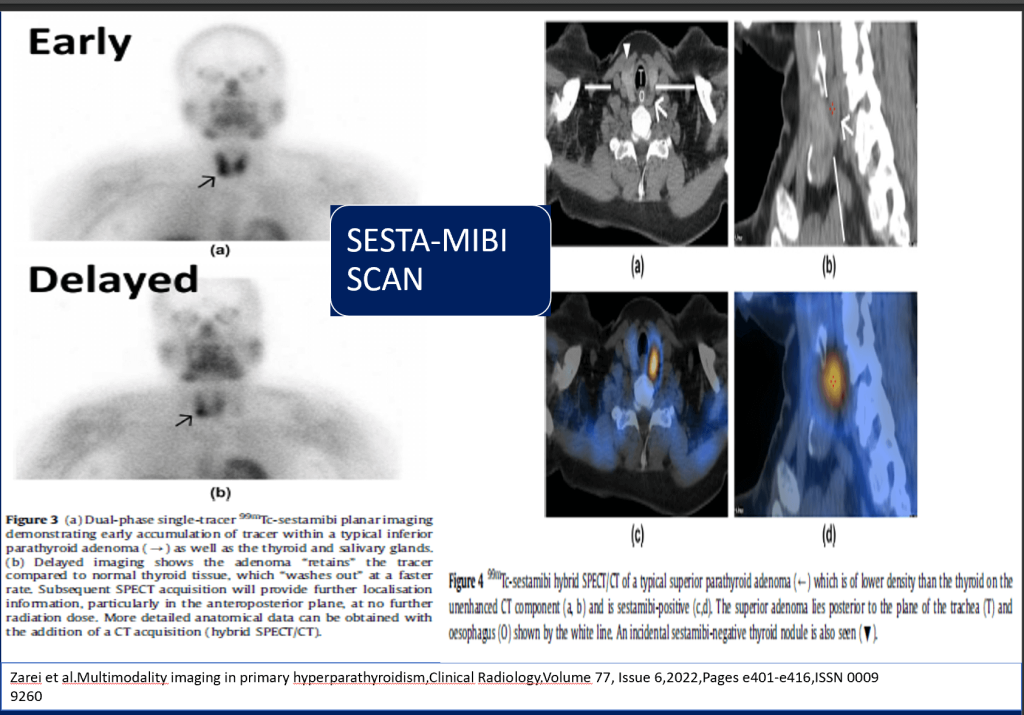
- Localization: Right inferior parathyroid adenoma by USG and Sesta-MIBI scan
- Treatment: Removal of parathyroid adenoma
- Normalization of calcium and PTH
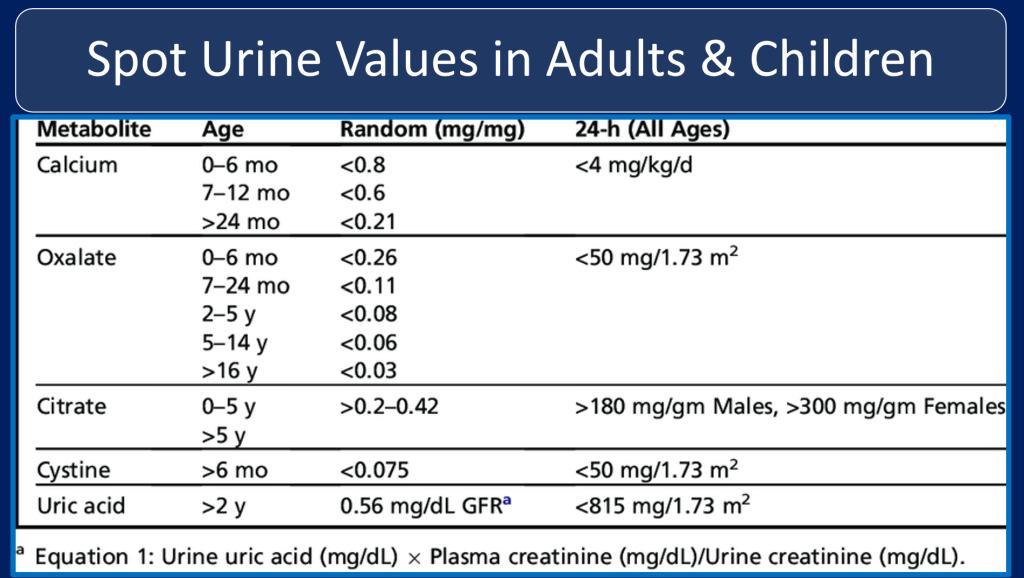
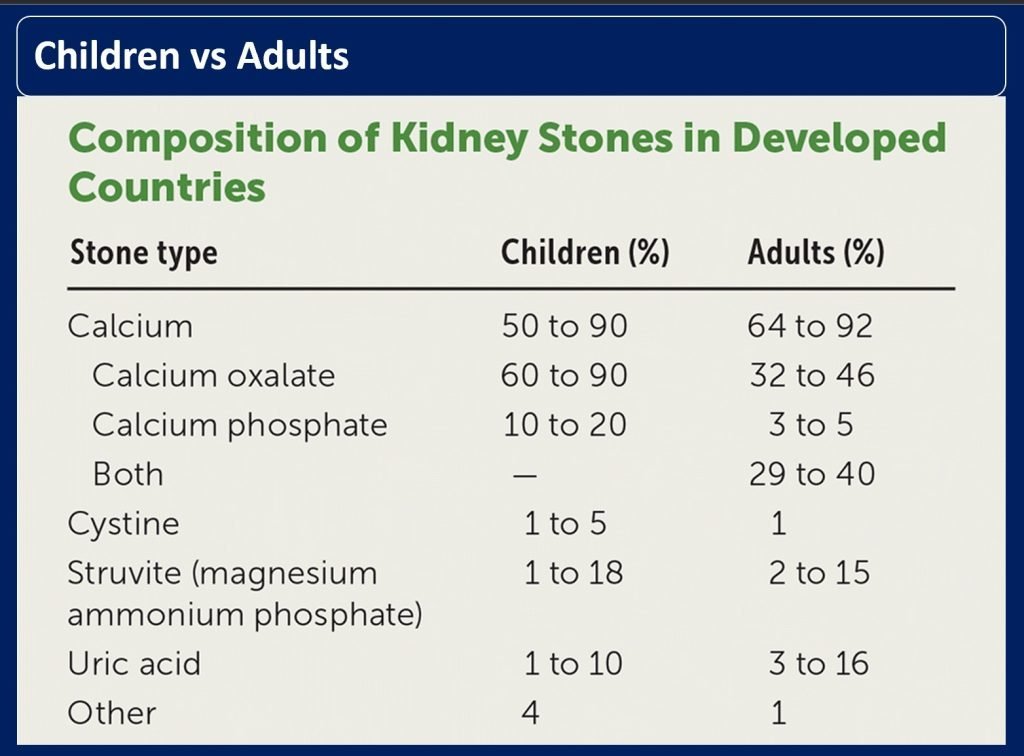
Children vs Adults
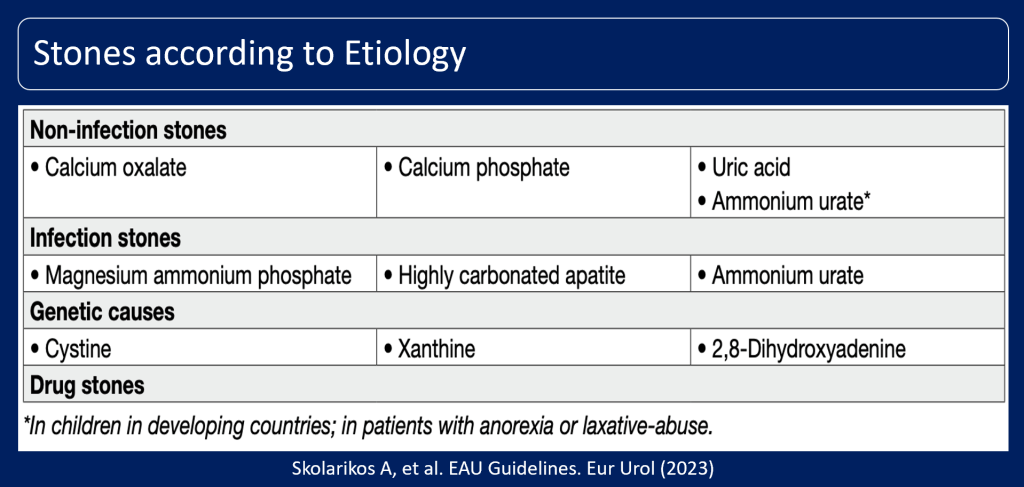
Stones according to Etiology
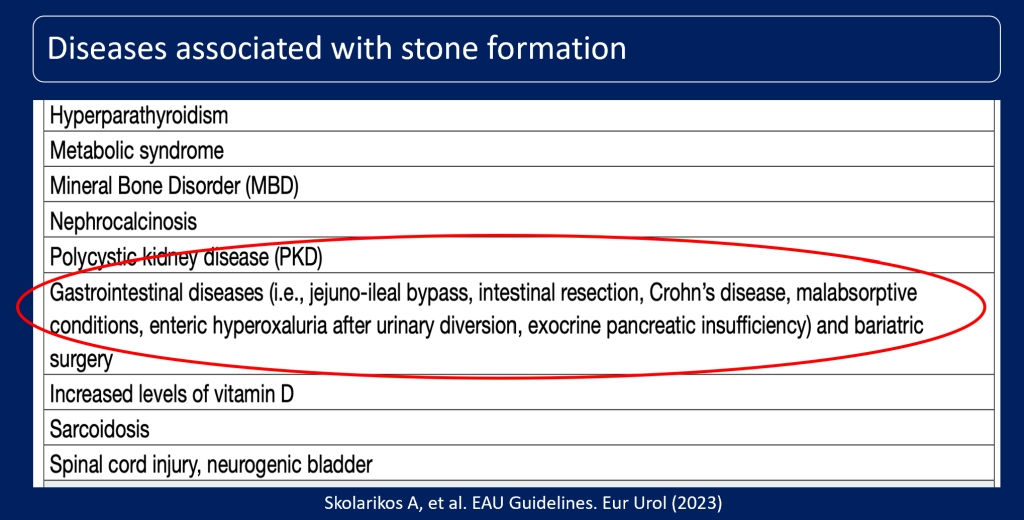
Diseases associated with stone formation
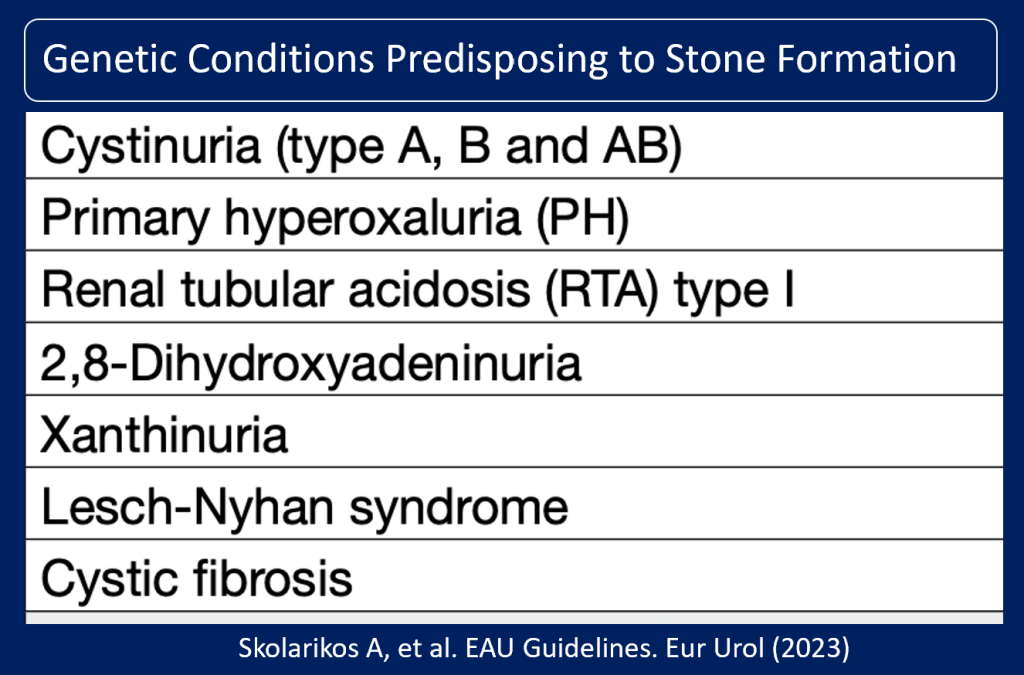
Genetic Conditions Predisposing to Stone Formation
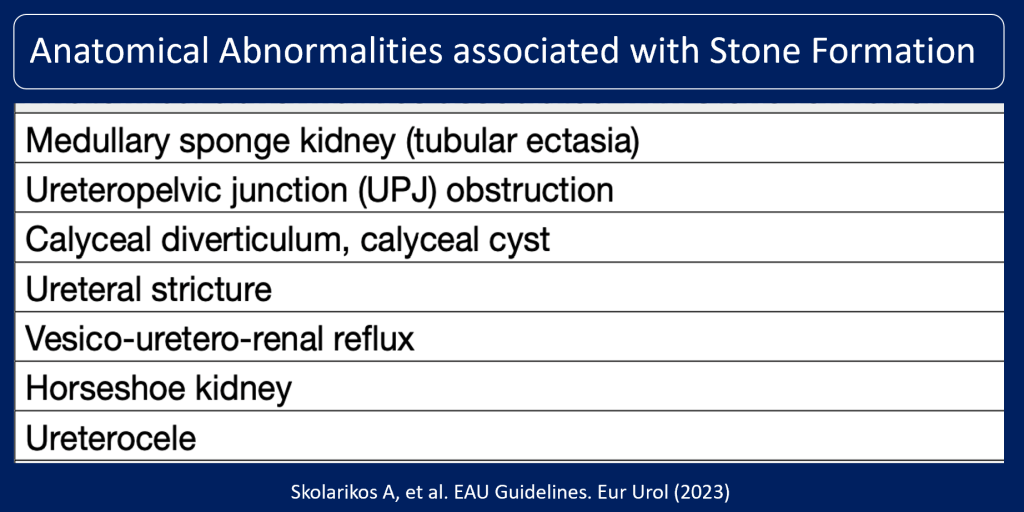
Anatomical Abnormalities associated with Stone Formation
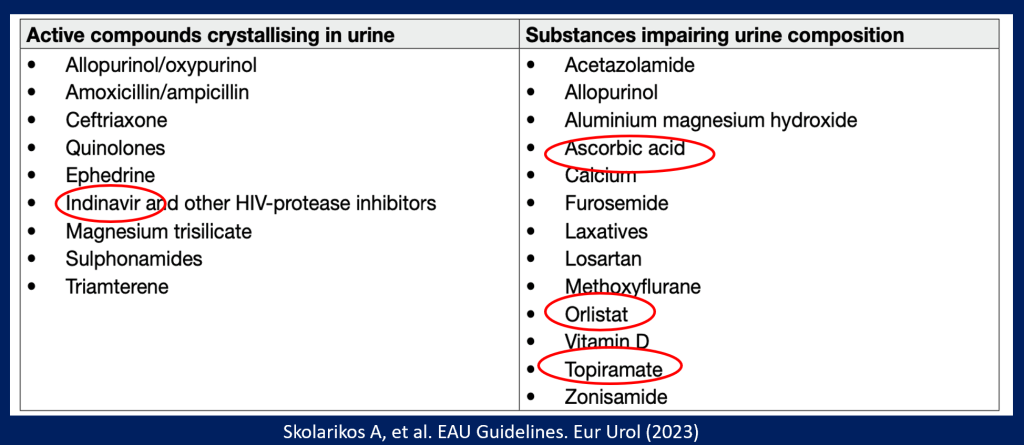
Compounds that cause drug stone formation
Occupational: High temperature and Lead/Cadmium exposure
- The development of nephrolithiasis in workers exposed to cadmium has been documented, with studies suggesting that individuals who are susceptible may develop kidney stones following damage to the renal tubular cells.
- Specifically, a clinical case study described a male worker who developed a Fanconi-like syndrome due to high exposure to cadmium fumes and subsequently showed evidence of nephrolithiasis with calcium phosphate stones ten years after his exposure was removed.
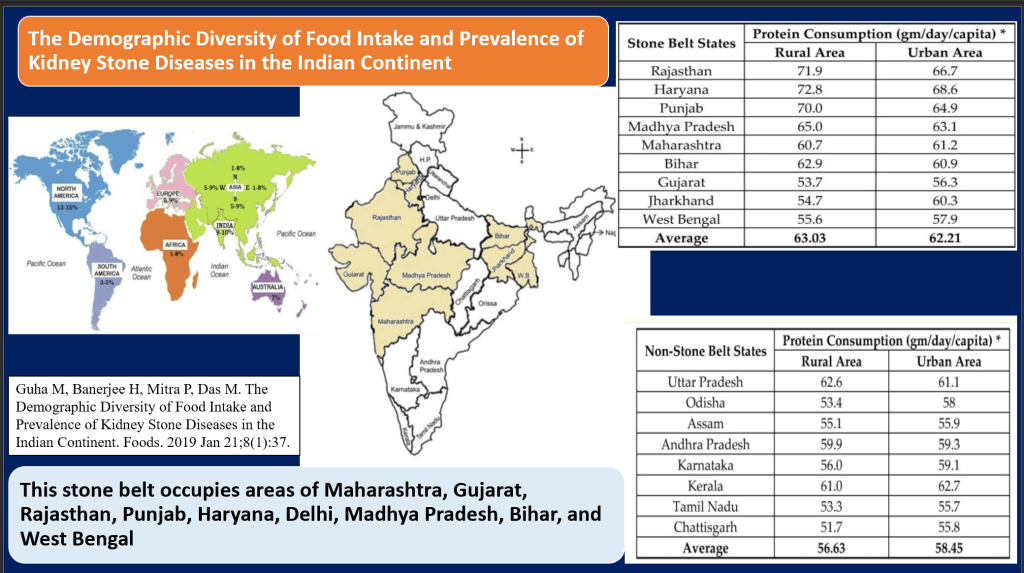
Link Between Dietary Diversity and Kidney Stone Prevalence Across India
- Dietary Influence: In India, diets high in protein and carbohydrates, particularly in the “stone belt” regions, correlate with higher kidney stone disease (KSD)rates. Dietary management could reduce recurrence, improving life quality.
- Pathogenic Mechanisms: Stone formation involves calcium imbalance due to renal leaks, excessive absorption, or bone issues, and mineralization. Key genes like VDR, CLDN-14, MGP, and SPP1 play roles in stone formation.
- Genetic and Molecular Insights: There’s a genetic predisposition in the Indian population, with genes influencing calcium and crystal aggregation. However, there are conflicting studies.
Treatment algorithm for renal stones (if/when active treatment is indicated)
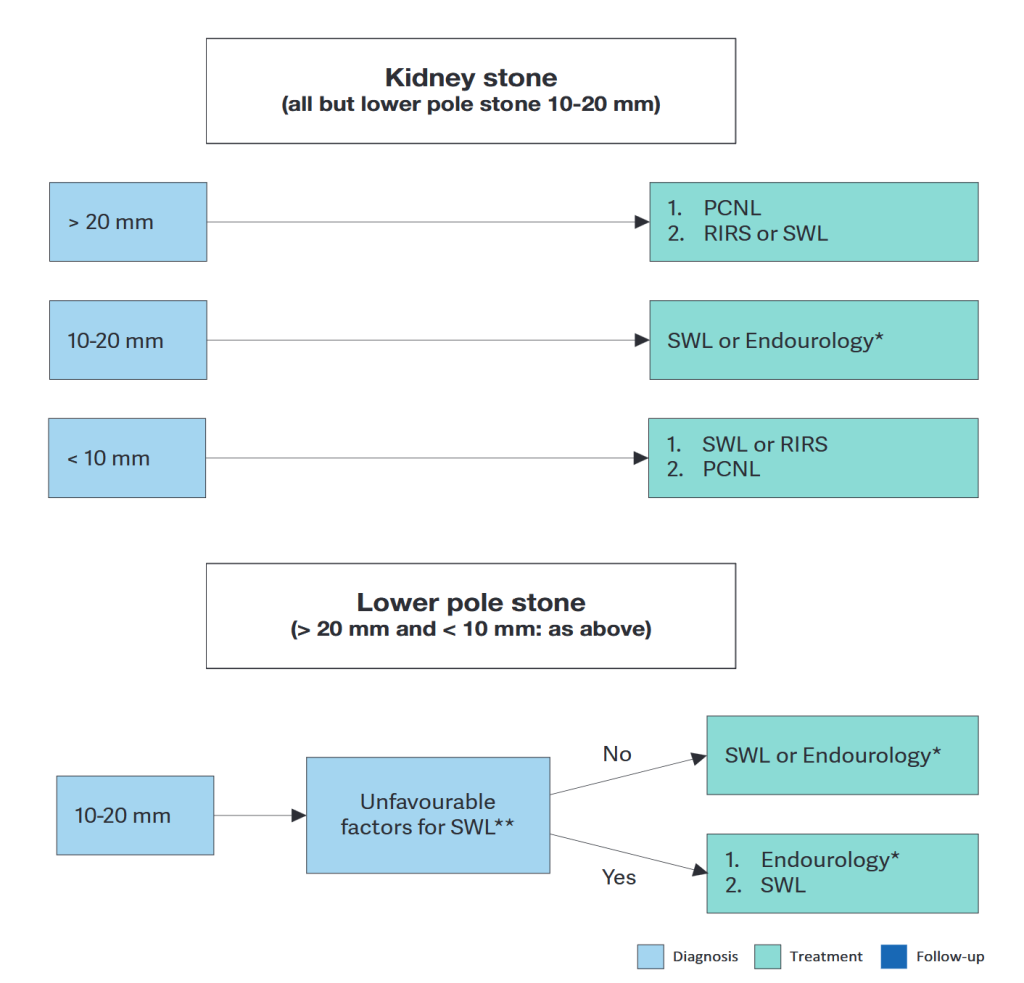
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Therapeutic algorithm for calcium oxalate stones
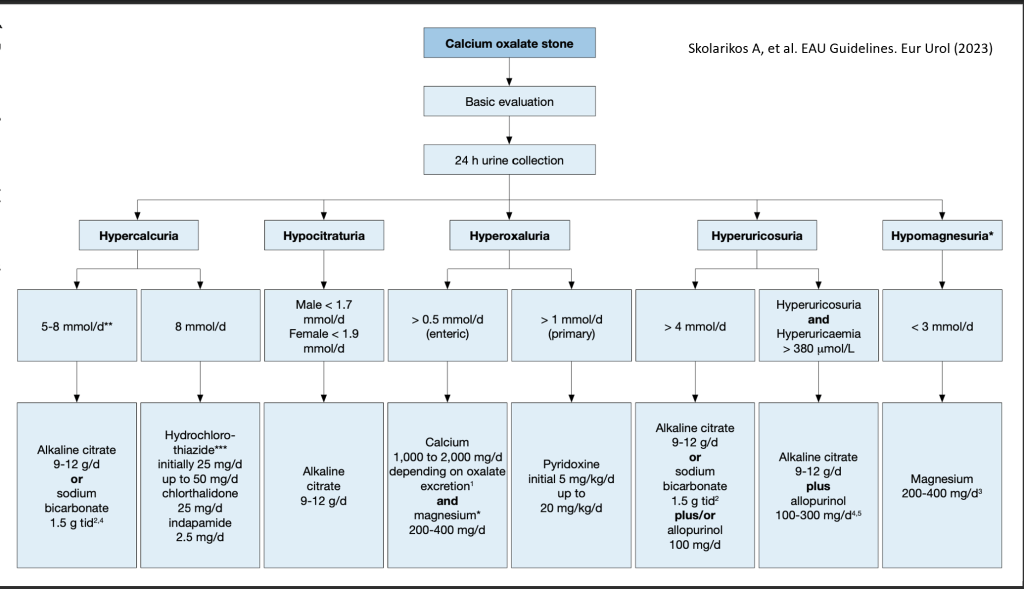
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Diagnostic and therapeutic algorithm for calcium phosphate stones
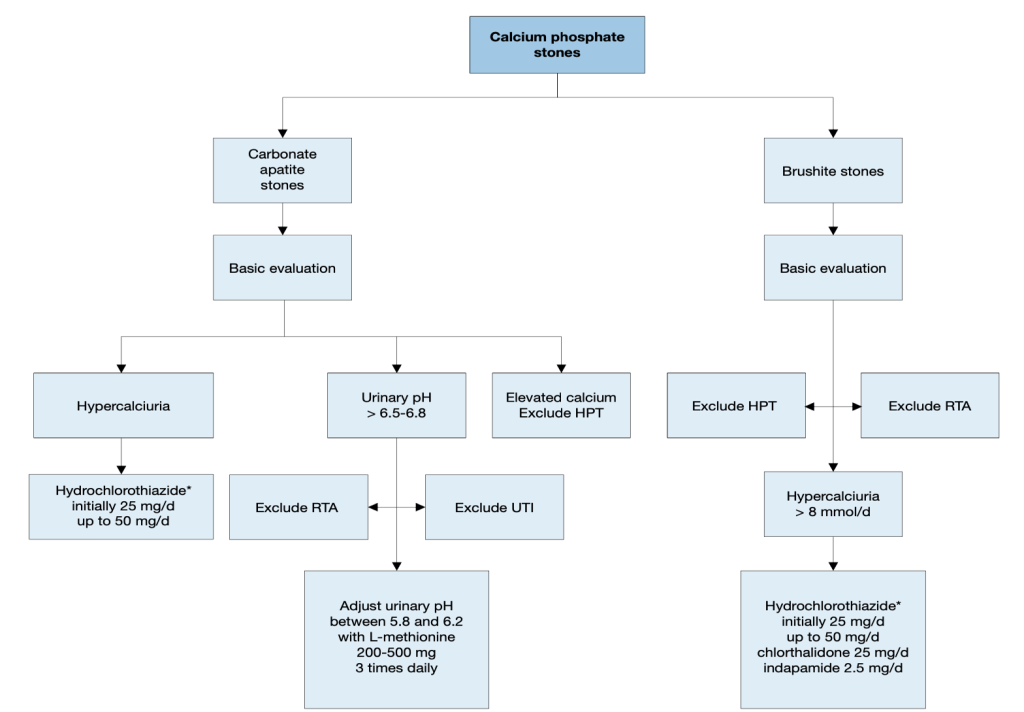
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Diagnostic algorithm for uric acid stones
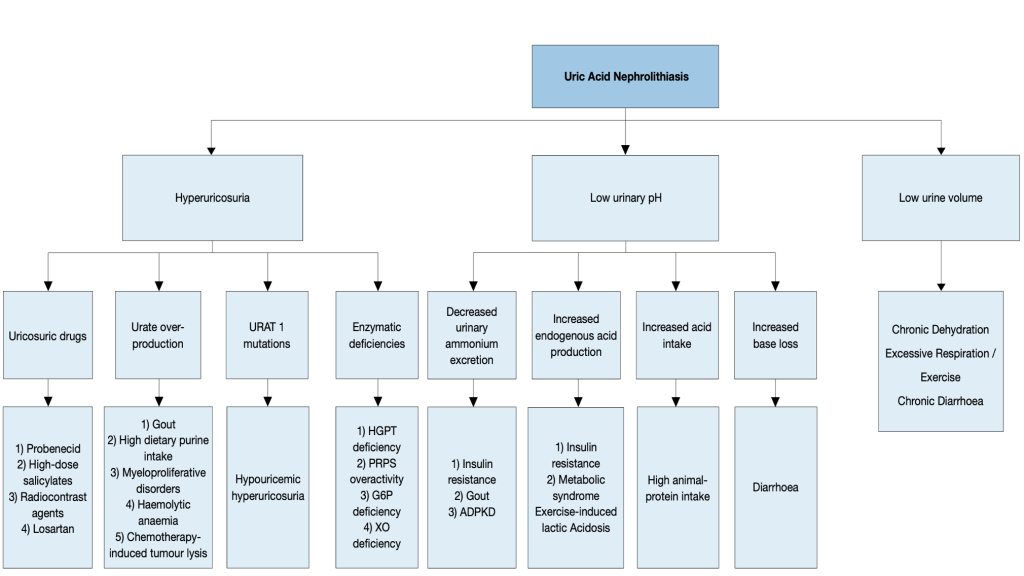
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Therapeutic algorithm for uric acid- and ammonium urate stones
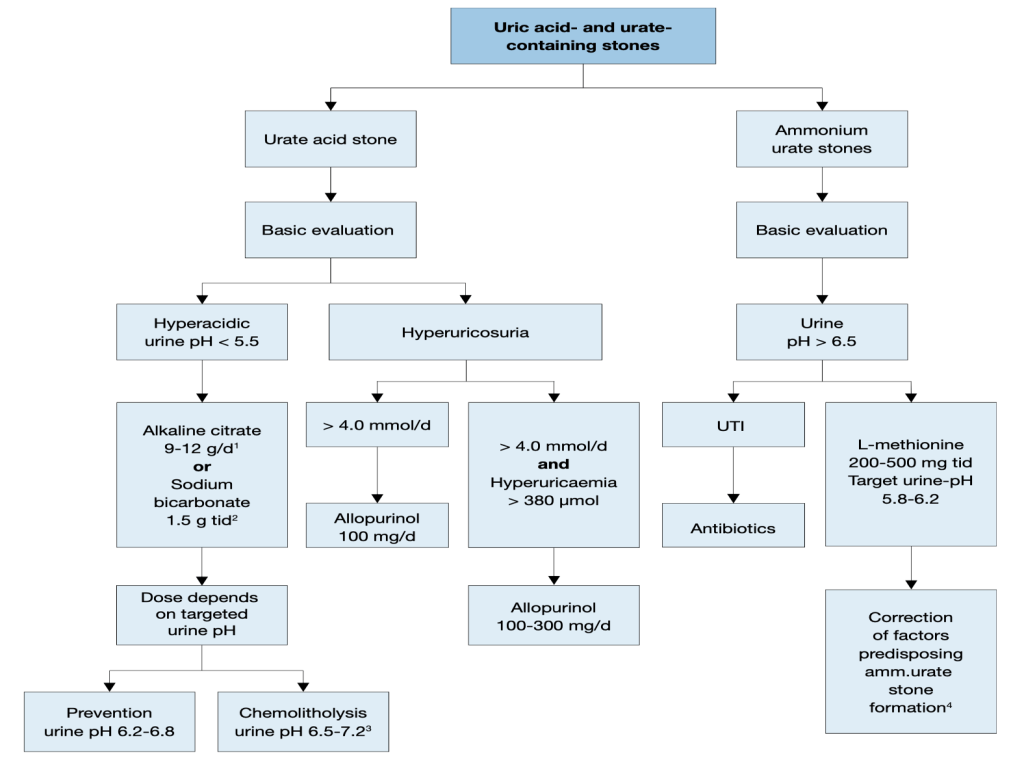
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Recommendations
- Prescribe alkaline citrates to alkalinise the urine in uric acid stone formers. (Strong)
- Prescribe allopurinol in hyperuricosuric urate stone formers. (Strong)
Should stone formers be given calcium supplements?
- Intestinal calcium absorption is likely different between stone formers and non-stone formers, with higher levels of calcium absorption in those with a history of stones independent of their calcium intake.
- Dietary calcium restriction is not recommended, as this may lead to bone demineralization and an increase in stone formation
- The effect of calcium supplementation on stone formation is currently controversial. It is likely that large doses of supplemental calcium, especially if taken separate from a meal, may lead to stone formation.
- When necessary, stone forming patients should be encouraged to take their calcium supplements with a meal and their stone disease should be monitored.
Pharmacological treatments for patients with specific abnormalities in urine composition (based on 24-hour urine samples)
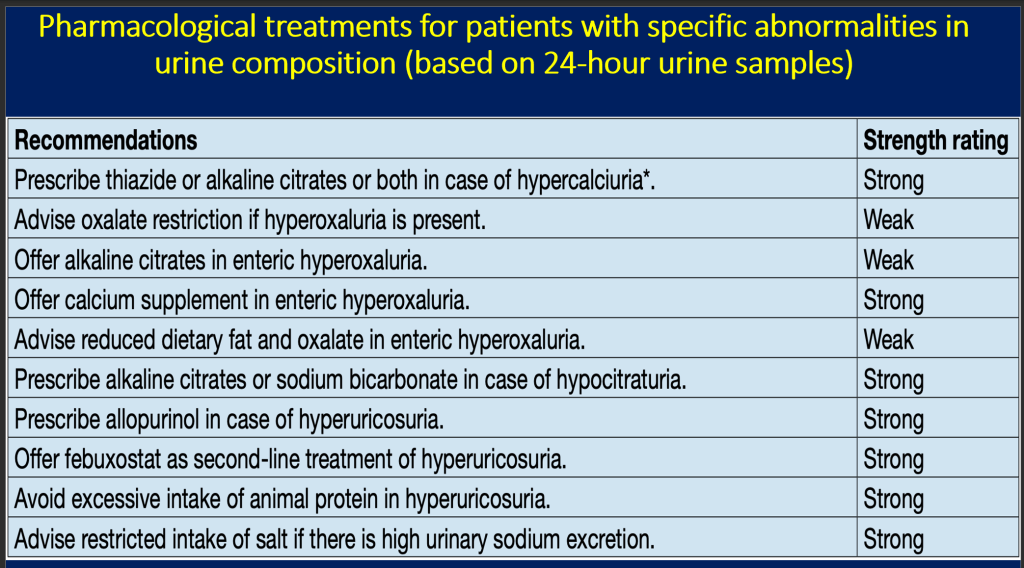
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
Final Points
| 5-10% lifetime chance of renal stone disease |
| First stone – at least basic investigation |
| Recurrent stone proper evaluation |
| Many treatable causes which are often ignored |
CME INDIA Must Know Points
Diet:
- General Advice: Adopt a balanced diet from all food groups without excesses. Ensure adequate calcium, particularly for vegetarians and vegans.
- Fruits, Vegetables, and Fiber: Promote intake for fiber benefits, though its preventive role in stone recurrence is unclear. These foods contribute to urinary alkalinity and hydration.
- Oxalate: Limit foods high in oxalate to manage oxalate load in susceptible individuals.
- Vitamin C: Its role in stone formation is debated; excessive intake should be avoided by those with calcium oxalate stones.
- Animal Protein: Limit to 0.8-1.0 g/kg body weight to avoid conditions like hypocitraturia and hyperoxaluria that promote stone formation.
- Calcium: Do not restrict without reason; maintain 1,000-1,200 mg daily. Supplements are advised only for specific conditions like enteric hyperoxaluria, with adequate fluid intake for older adults taking supplements.
- Sodium: Keep intake below 4-5g daily to prevent increased calcium excretion, reduced citrate, and sodium urate crystal formation. Sodium restriction’s role in preventing stones is clearer in women but lacks strong prospective evidence.
- Urate: Restrict purine-rich foods to below 500 mg/day for those with hyperuricosuric calcium oxalate or uric acid stones.
Diagnostic Evaluation:
- Diagnostic Imaging:
- The choice of imaging depends on whether a ureteral or renal stone is suspected.
- Initial evaluation includes medical history and physical exam.
- Ureteral Stones: Present with symptoms like loin pain, vomiting, and sometimes fever; immediate evaluation needed for solitary kidney or fever cases.
- Ultrasound (US): Primary imaging choice; safe, reproducible, and cost-effective. Identifies stones in various locations with sensitivity/specificity of 45%/94% for ureteral stones and 45%/88% for renal stones.
- KUB Radiography: Sensitivity and specificity range from 44-77%. Useful for distinguishing between radiolucent and radiopaque stones, aiding in follow-up comparisons.
Evaluation of Patients with Acute Flank Pain/Suspected Ureteral Stones:
- Non-Contrast-Enhanced Computed Tomography (NCCT): Has become the standard diagnostic tool for acute flank pain, replacing intravenous urography (IVU). NCCT identifies stone location, size, and density.
- Accuracy: NCCT is significantly more accurate than IVU or ultrasound for diagnosing acute urolithiasis.
- Stone Detection: NCCT can detect radiolucent stones like uric acid and xanthine, but not indinavir stones. It provides information on stone structure, density, and anatomical context, guiding treatment choices.
- Drawbacks: NCCT does not provide information on renal function or detailed anatomy of the urinary collecting system, and it involves a higher radiation dose.
- Radiation Reduction: Low-dose CT offers a way to reduce radiation exposure while maintaining high diagnostic accuracy, particularly effective for patients with BMI < 30. A meta-analysis shows low-dose CT has 93.1% sensitivity and 96.6% specificity for diagnosing urolithiasis.
- Dual-Energy CT: Allows differentiation between uric acid and calcium-containing stones, enhancing diagnostic specificity.
Recommendations in Pregnancy
- Use ultrasound as the preferred method of imaging in pregnant women. (Strong)
- Use magnetic resonance imaging as a second-line imaging modality in pregnant women. (Strong)
- Use low-dose computed tomography as a last-line option in pregnant women. (Strong)
Always Do Analysis of Stone Composition:
- Recommendation: Stone analysis should be conducted for all first-time stone formers.
- Repeat Analysis: Necessary in cases of:
- Stone recurrence despite pharmacological prevention.
- Early recurrence post-interventional therapy with complete stone clearance.
- Late recurrence after a significant stone-free period.
- Procedure: Patients should filter their urine to collect stones for analysis, confirming stone passage and return to baseline renal function.
- Analytical Methods:
- Infrared Spectroscopy (IRS) and X-ray Diffraction (XRD) are the preferred methods for stone analysis.
- Polarization microscopy can yield equivalent results.
- Wet chemistry or chemical analysis is considered outdated.
Medical Expulsive Therapy (MET): Myth or Reality?
- Drugs Used: α-blockers, calcium channel inhibitors, and phosphodiesterase type 5 inhibitors (PDEI-5) are employed for MET.
- α-Blockers:
- Meta-analyses have shown a class effect for α-blockers in MET, though this is off-label.
- However, there are conflicting results from well-designed studies, with some showing limited or no benefit, except perhaps for distal ureteral stones > 5 mm.
- PDEI-5 and Corticosteroids: Current evidence does not support the use of these drugs in combination with α-blockers due to limited patient studies.
- Conclusion: α-blockers appear effective for MET in patients with distal ureteral stones > 5 mm suitable for conservative management. ( Alpha-blockers are an off-label treatment)
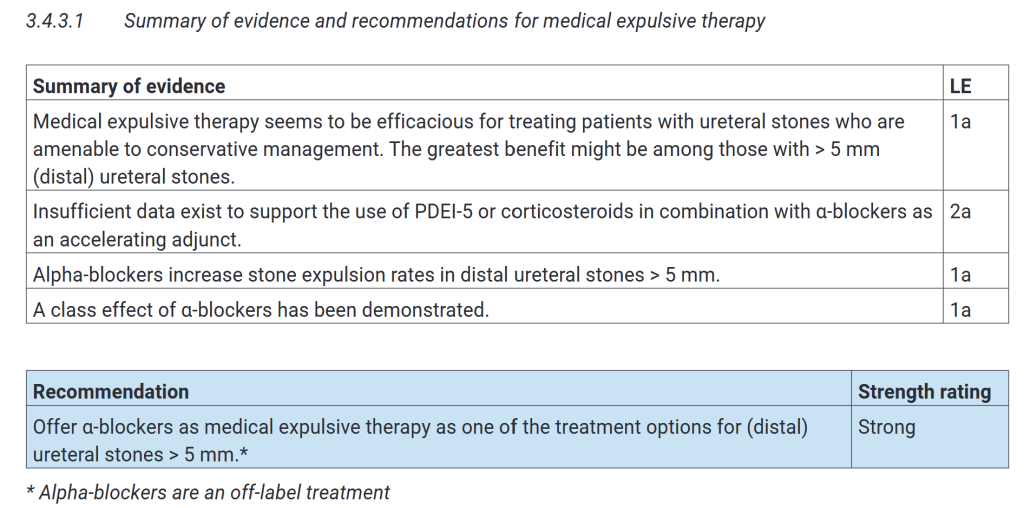
Courtesy: Skolarikos A, et al. EAU Guidelines. Eur Urol (2023)
What about Oral Chemolysis?:
- Target Stones: Effective for dissolving uric acid stones, not sodium or ammonium urate stones.
- Pre-treatment Assessment: Stone analysis, urinary pH, and X-ray characteristics help determine stone type.
- Method: Involves alkalinizing urine with alkaline citrate or sodium bicarbonate, aiming for a pH of 7.0-7.2. Higher pH enhances dissolution but risks calcium phosphate stone formation.
- Patient Management: Patients adjust medication based on self-monitored urine pH.
- Effectiveness: A systematic review indicates an 80.5% success rate in complete or partial dissolution, with a 10.2% discontinuation rate and 15.7% needing further intervention.
- Special Cases: For uric acid obstruction, combining oral chemolysis with urinary drainage is advised. Adding tamsulosin can increase spontaneous passage rates for distal ureteral uric acid stones > 5 mm according to one RCT.
- Additional Treatment: Combining with shock wave lithotripsy (SWL) may improve outcomes, though evidence is limited
Extracorporeal Shock Wave Lithotripsy (SWL):
- Success Factors:
- Stone Characteristics: Size, location, and composition (hardness) of the stone.
- Patient’s Habitus: Physical condition of the patient.
- Performance of SWL: Adherence to best clinical practices.
- Best Clinical Practice:
- Stenting: Routine use of internal stents prior to SWL does not enhance stone-free rates or reduce the need for additional treatments. However, it may help prevent steinstrasse (stone street formation).
Pacemaker Considerations for SWL:
- Pacemaker Patients: Can undergo SWL if technical precautions are followed.
- Implanted Cardioverter Defibrillators (ICDs): Require special management, with the firing mode temporarily reprogrammed during SWL. This precaution might not be necessary with newer generation lithotripters.
Antibiotic Prophylaxis for SWL:
- General Recommendation: Standard antibiotic prophylaxis is not recommended before SWL.
- Specific Cases: Prophylaxis is advised when:
- There’s an internal stent placement prior to treatment.
- There’s an increased bacterial burden (e.g., indwelling catheter, nephrostomy tube, or presence of infectious stones).
Medical Therapy Post-SWL:
- Medical Expulsion Therapy (MET): Despite some conflicting data, most randomized controlled trials (RCTs) and meta-analyses (MAs) endorse MET following SWL for ureteral or renal stones. It may:
- Speed up stone expulsion.
- Increase stone-free rates (SFRs).
- Reduce the need for analgesics.
References:
- Goyal T, Mitra P, Singh P, Sharma S, Sharma P. Assessement of Blood Lead and Cadmium Levels in Occupationally Exposed Workers of Jodhpur, Rajasthan. Indian J Clin Biochem. 2021 Jan;36(1):100-107. doi: 10.1007/s12291-020-00878-6. Epub 2020 Mar 14. PMID: 33505134; PMCID: PMC7817726.
- Trevisan A, Gardin C. Nephrolithiasis in a worker with cadmium exposure in the past. Int Arch Occup Environ Health. 2005 Sep;78(8):670-2. doi: 10.1007/s00420-005-0009-z. Epub 2005 Oct 12. PMID: 16001205.
- Guha M, Banerjee H, Mitra P, Das M. The Demographic Diversity of Food Intake and Prevalence of Kidney Stone Diseases in the Indian Continent. Foods. 2019 Jan 21;8(1):37. doi: 10.3390/foods8010037. PMID: 30669549; PMCID: PMC6352122.
- A.Skolarikos (Chair), H. Jung, A. Neisius, A. Petřík, B. Somani etal. European Association of Urology 2024.
- Sorensen MD. Calcium intake and urinary stone disease. Transl Androl Urol. 2014 Sep;3(3):235-40. doi: 10.3978/j.issn.2223-4683.2014.06.05. PMID: 26816771; PMCID: PMC4708574.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
We stress on more water intake in stones.Does कुर्ती का पानी have any role?