

CME INDIA Presentation by Dr. Vijay KR Rao,MBBS, MRCP (UK), MRCP (UK) Rheum CCT Rheum (UK), FRCP Edin (UK), Consultant Rheumatologist and clinical director at Divisha Arthritis And Medical Center, Bangalore.
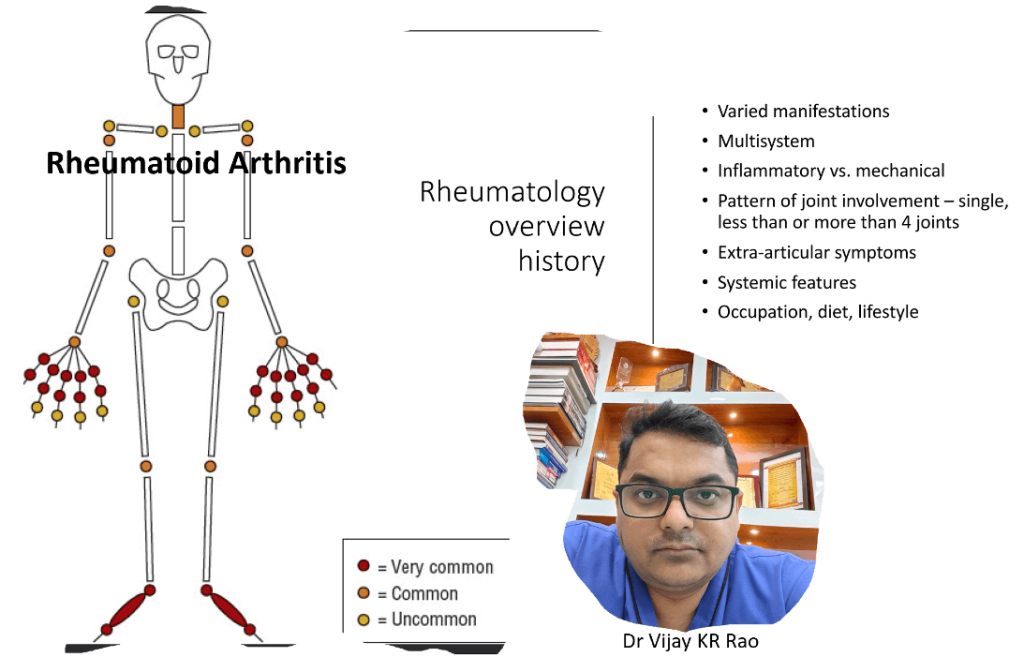
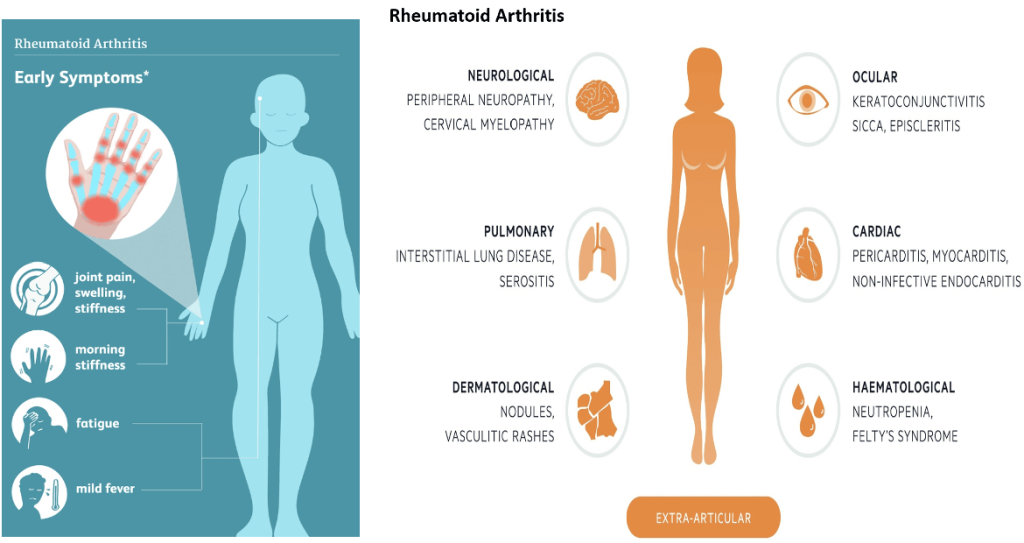
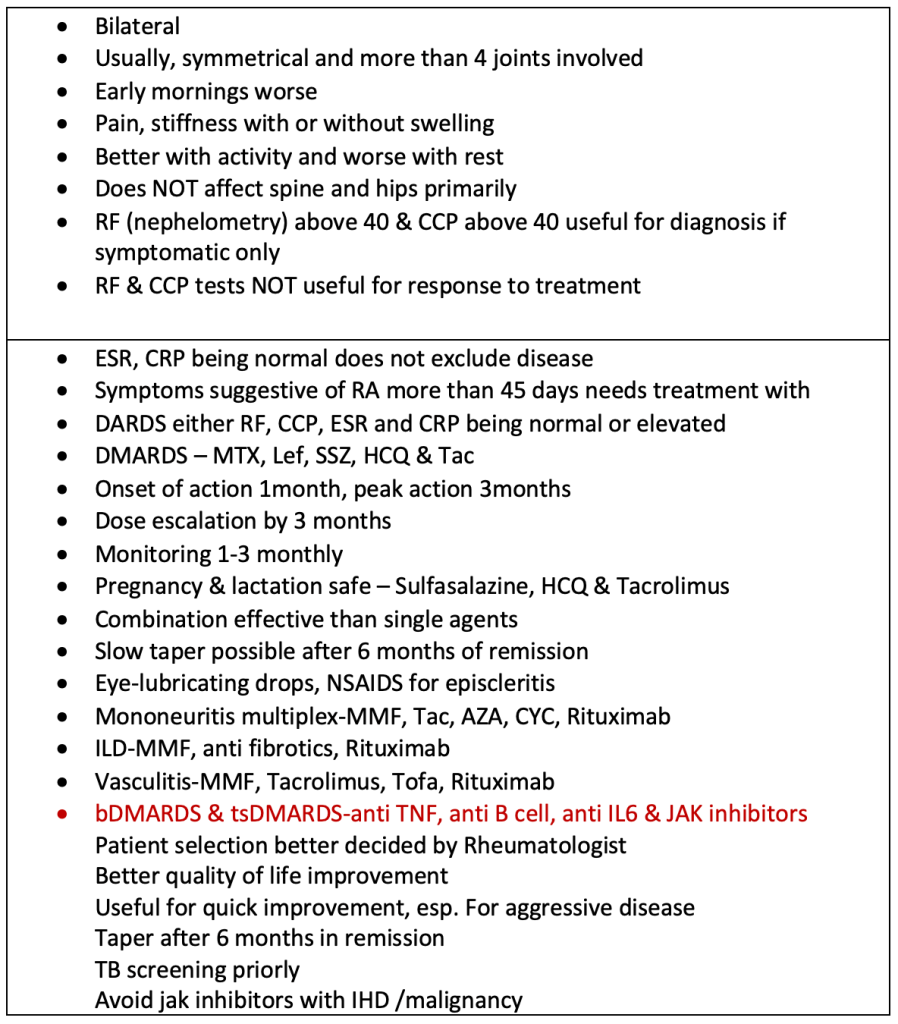
Rheumatoid Arthritis (RA)
Seronegative arthritides (SpA)
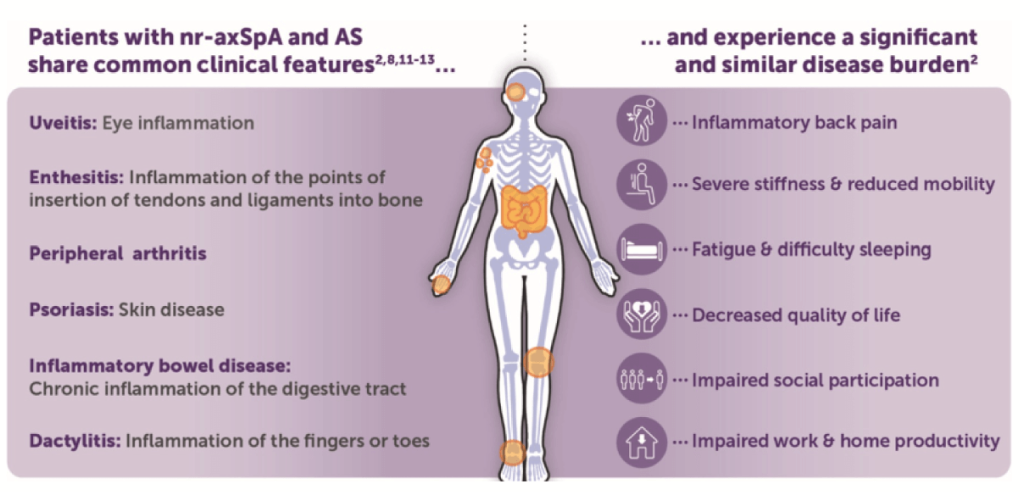
Ankylosing spondylitis (eye, peripheral arthritis & spinal arthritis)
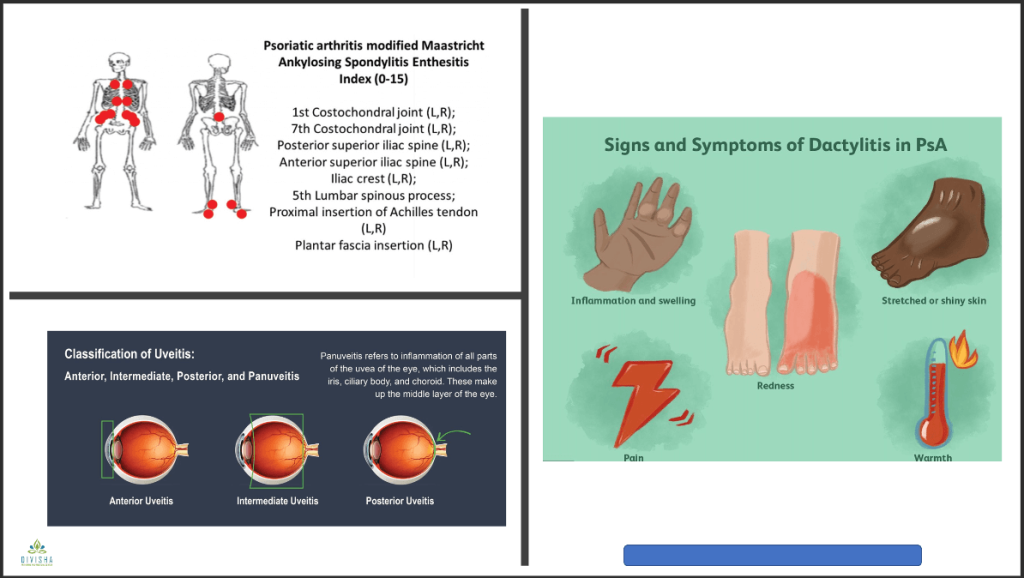
- Psoriatic disease (eye, skin, nails, peripheral arthritis & spinal arthritis)
- Enteropathic arthritis (IBD arthritis)
- Reactive arthritis (GI/GU infection first & then inflamed joints+/-eye+/-urethra)
- Undifferentiated variety
Mostly a clinical diagnosis
- ESR, CRP normal in 40% cases – does not exclude SpA
- HLAB27 positivity varies – 50% in AS in Indians, 25% in PsA
- MRI evidence of inflammation seen mostly in spinal disease
- X ray useful for peripheral joints – hands, feet, knees, pelvis
- All are NSAIDS responsive
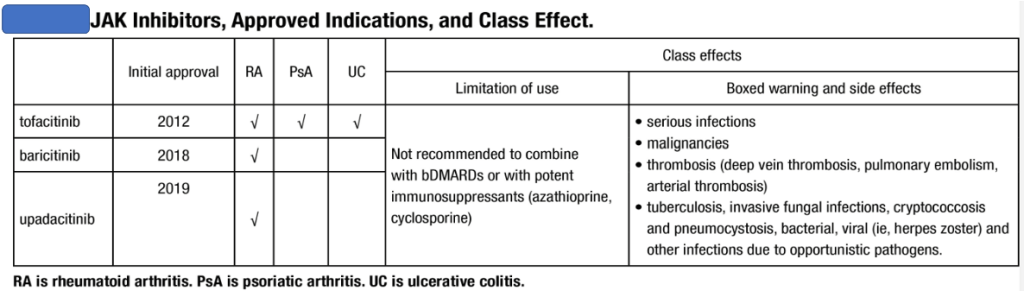
- csDMARDS & tsDMARDS 70% responsive – MTX, SSZ(enthesitis, spinal), Lef, Tofa, apremilast (Psoriasis)
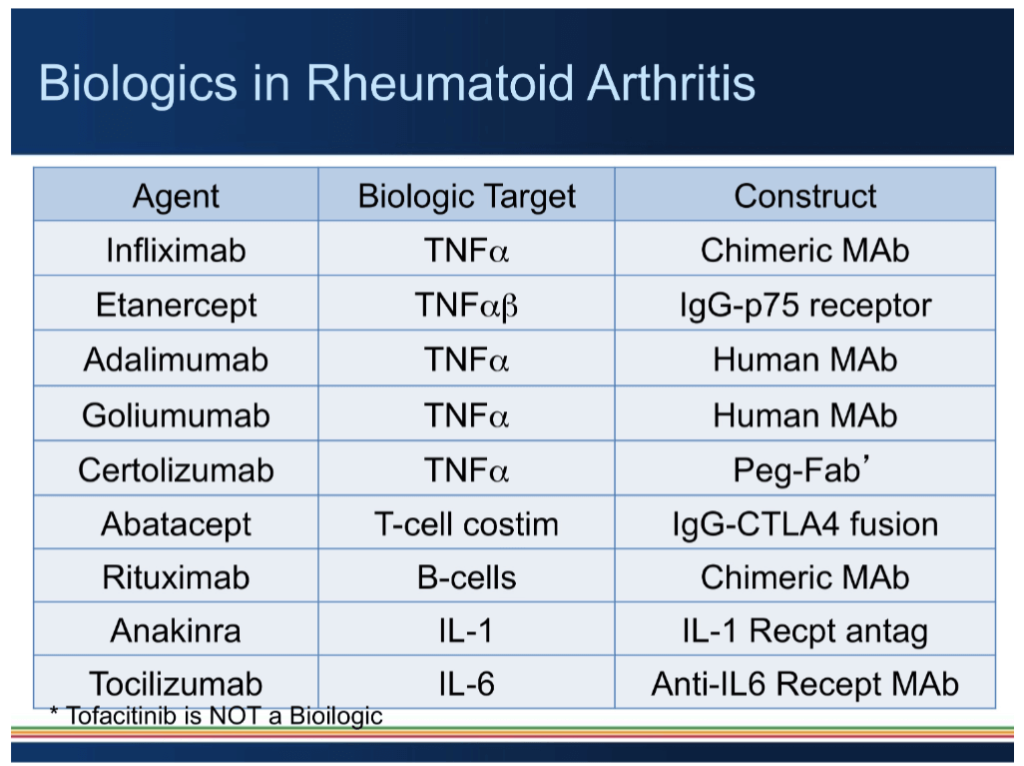
- bDMARDS – resistant, severe, spinal, young, uveitis & IBD patients
- Anti TNF (skin, nails, joints, spine, entheses, eyes & IBD) anti IL17 pathways (skin predominant)
Connective tissue diseases (CTD)
| Commonly seen – UCTD, SLE, Sjogren’s, MCTD, overlap CTD, autoimmune myositis, Scleroderma |
| • Mostly have anti-nuclear or anti cytoplasmic antibodies |
| • ANA IF (dilution titre) and or ANA profile antibodies are strongly positive |
| • Usually, multi system symptoms & evolving even with treatment |
| • Treatment varied based on symptoms, severity and type of organ involved |
CTD – Organ specific treatments
- Joints – MTX, Tofa, Tacrolimus
- Brain (NPSLE) – CYC, MMF, Rituximab
- Eyes (uveitis, retinal vasculitis, scleritis) – CYC, MMF, Rituximab
- Serositis (lupus pleuro, pericardial effusion, ascites) – AZA, MMF, Tacrolimus, Rituximab
- Lungs – ILD (Scleroderma, myositis, MCTD) MMF, Rituximab, Tacrolimus, Tofa
- GI (lupus bowel vasculitis) – CYC,MMF, RituximabHaemat (lupus pancytopenia, ITP,AIHA, MAS-HLH) – AZA, MMF, Tacrolimus, Rituximab, IV immunoglobulins
- Muscles (Myositis) – MTX, MMF, Tofa, Tacrolimus, CYC, Rituximab
- Renal (SLE) – MMF, Tacrolimus, CYC,Rituximab
- Skin (SLE, Scleroderma, Myositis)AZA, MMF, Tacrolimus, Tofa, CYC, Rituximab
- Peripheral nerve (Sjogren’s) – MMF, Tacrolimus, CYC, Rituximab
CTD – Adjunctive treatments
All SLE patients need HCQ treatment unless contraindicated
- Steroids – if moderate CTD (0.25-0.5mg/kg/d tapering); if severe (renal/neuro – 0.5-1mg/kg/d tapering); aim for less than 5mg/d by 3 months
- APLA profile and subsequent anticoag (lupus anticoag+antiB2GP+antiACL) – check if arterial/venous thromboses/recurrent EPL)
- Eye lubricants & salivary stimulants for sicca (oral & mouth dryness) symptoms
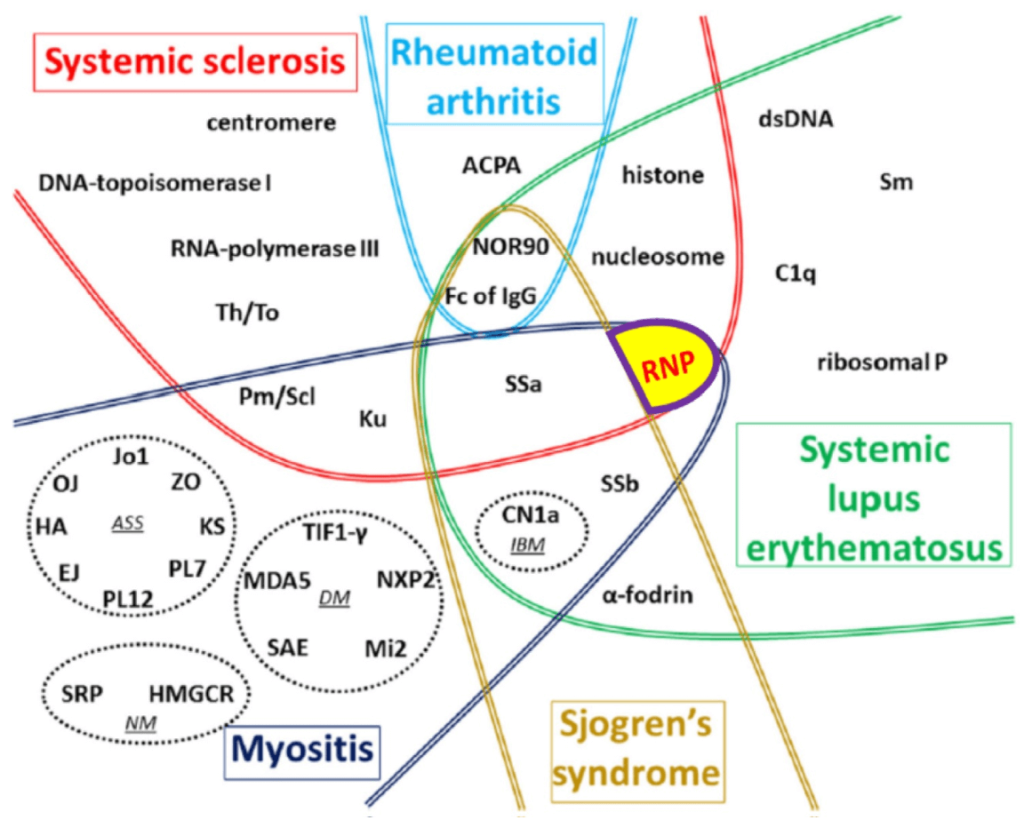
CTD – disease specific attributes
| • Low C3, anti sm & dsDNA (quantitative by ELISA) – SLE |
| • Anti RNP – MCTD, ILD |
| • Anti RNA polymerase 3 – scleroderma renal crisis |
| • Rashes on eyelids, necklace area & back of neck – dermatomyositis |
| • Pepper pot pigmentation on back of neck – Scleroderma |
| • Malar & photosensitive rash – SLE |
| • Microstomia & perioral puckering Scleroderma anti MDA5 – ILD associated with myositis |
| • Anti TIF1g – malignancy associated myositis |
| • Anti ribosomal P – neurological disease in CTD |
| • Digital pits & Raynaud’s – scleroderma |
| • PM-Scl – Overlap CTD |
| • SSA (Ro) & SSB (La) – Sjogren’s |
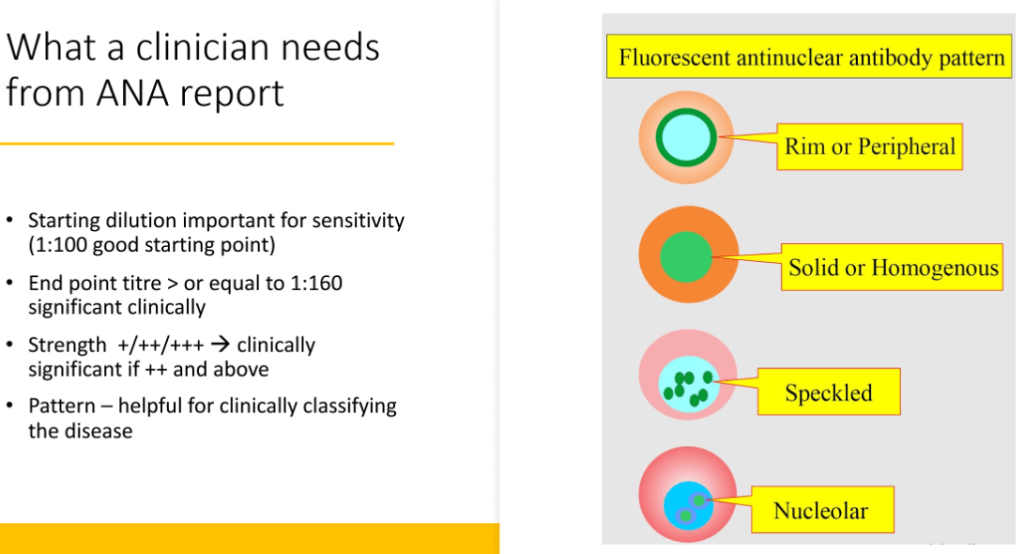
What a clinician needs from ANA report?
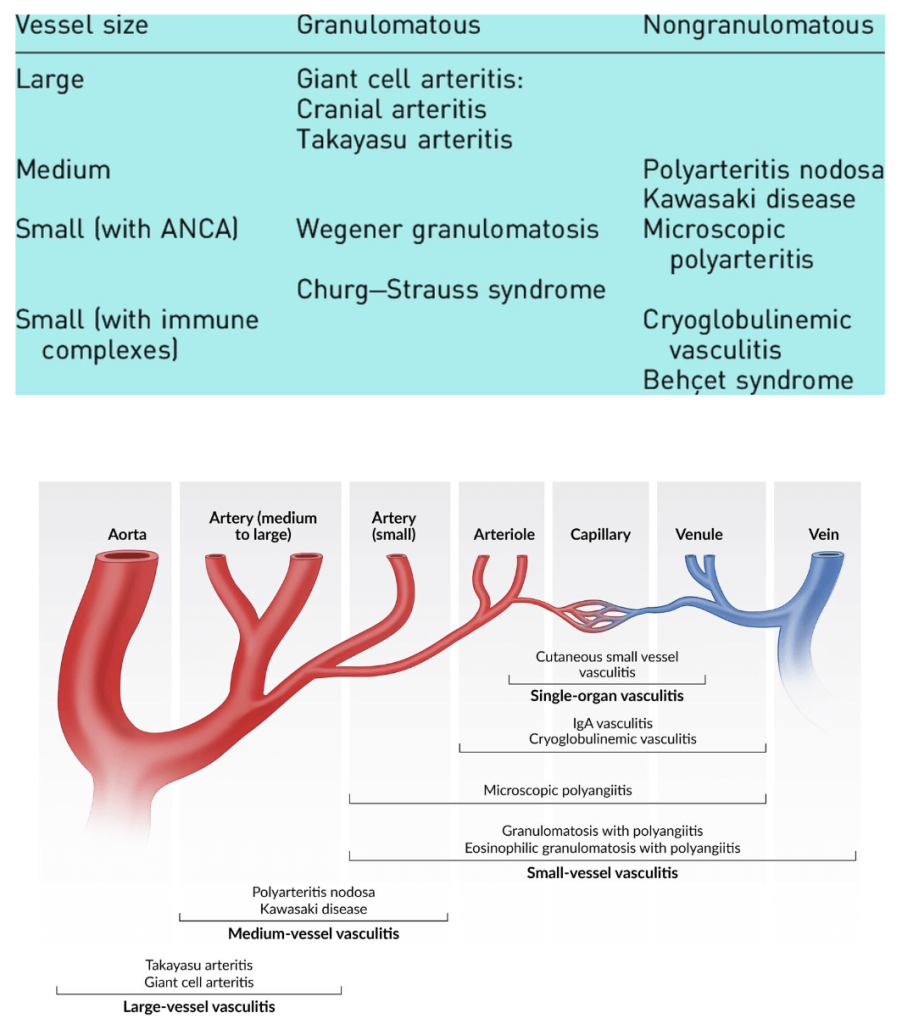
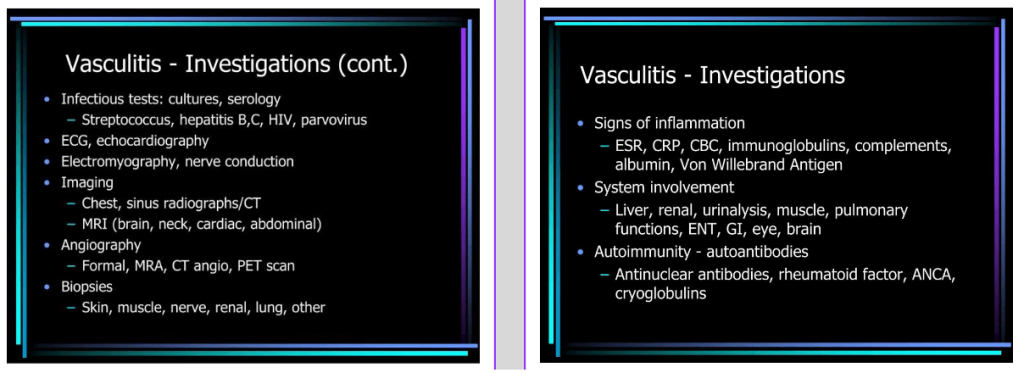
Vasculitides
| Varied symptoms |
| Pattern depends on size of vessel involved |
| Imaging mandatory for Large vessel vasculitis diagnosis |
| Biopsy necessary for medium and small vessel vasculitis |
| Life-threatening if major organs involved – brain, heart, lungs, intestines, kidneys |
| Always rule out differentials – infection |
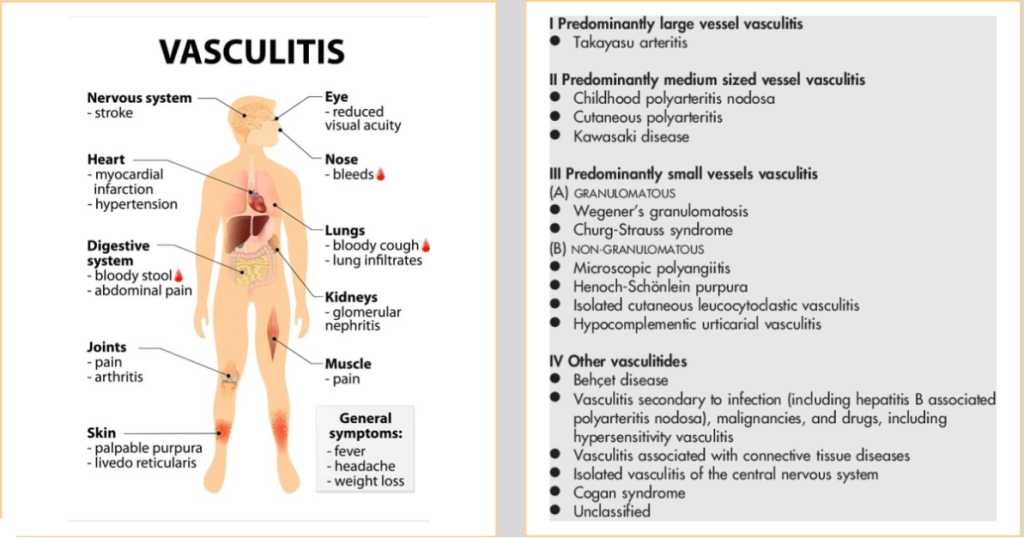
Credit: ©ttsz/iStock/Getty Images Plus
Vasculitis treatment
- Takayasu arteritis – prednisolone 1mg/kg/d tapering, MTX, MMF, anti IL6, anti TNF
- Giant cell arteritis – prednisolone 1mg/kg/d tapering, MTX, Lef, anti IL6, ANTI tnf
- Polyarteritis Nodosa (PAN) – prednisolone 1mg/kg/d tapering, CYC, RTX, AZA, MMF, Tofa
- Granulomatosis Polyangiitis (GPA) – Prednisolone 1mg/kg/d, CYC, RTX, AZA, MMF
- Microscopic Polyangiitis (MPA) – Prednisolone 1mg/kg/d, CYC, RTX, AZA, MMF
- IgA and other small vessel cutaneous vasculitis – prednisolone 0.5mg/kg/day tapering, MTX, AZA, MMF, Tofa
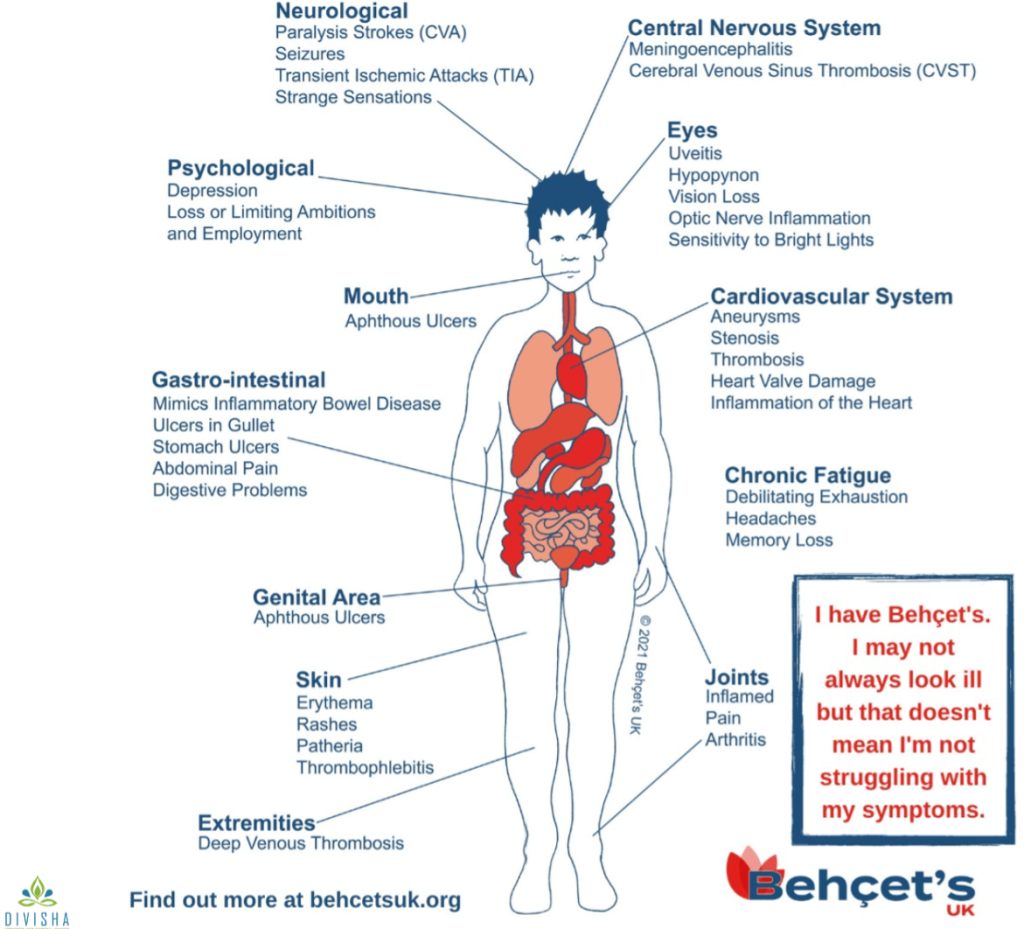
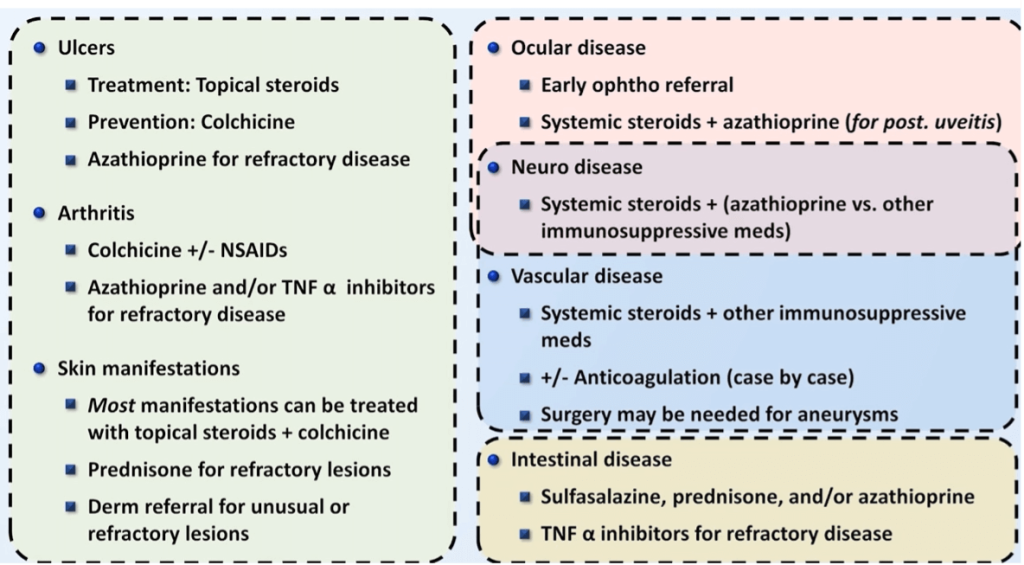
- Bechet’s – Prednisolone 0.5mg/kg/d, AZA, Ciclosporin, MMF, Anti TNF, apremilast, colchicine
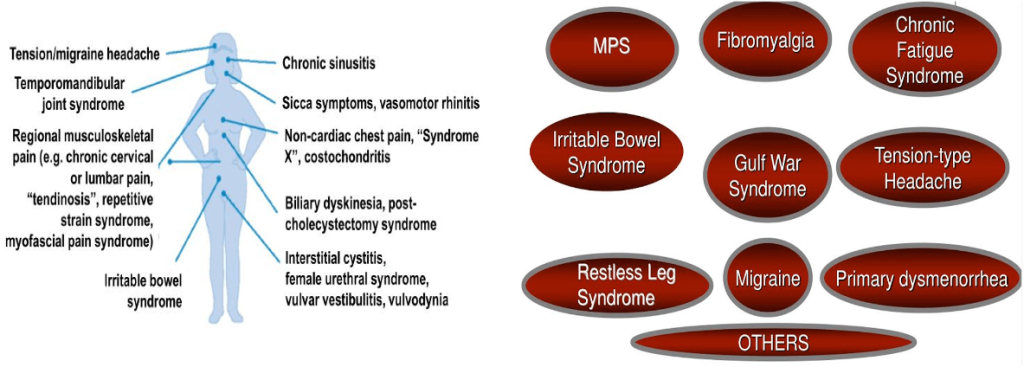
Common non inflammatory symptoms seen in clinic
Gout & hyperuricemia
High serum uric acid alone does not cause arthralgia/myalgia
| Gout is diagnosed by clinical presentation |
| • Acute arthritis in the coolest joint of the body (big toe) |
| • Usually, no symptoms between attacks |
| • More than 2 attacks/year needs uric acid lowering treatment |
| • 6 months of allopurinol/febuxostat |
| • NSAIDS/steroids/colchicine for acute attacks |
| • Asymptomatic high uric acid does not treatment or monitoring |
| • Low carbohydrate, low saturated fat, no seafood/no red meat, low/no alcohol, no processed foods |
| • 30 min of aerobic physical exercises per day |
Osteoporosis
Does not cause pain if there is no fracture
- Defined as osteoporosis when there is:
- Fragility low velocity fracture – hips/spine/wrist
- Or DEXA whole body scan T score -2.5 and beyond in either and hips, spine or wrist
- Or FRAX score overall fracture risk of more than 20% or hip fracture risk of more than 3%
- Teriparatide if fragility low velocity fracture seen
- Bisphosphonates, denosumab in osteoporosis without fracture
- Vit D prophylaxis if risk factors present for osteoporosis
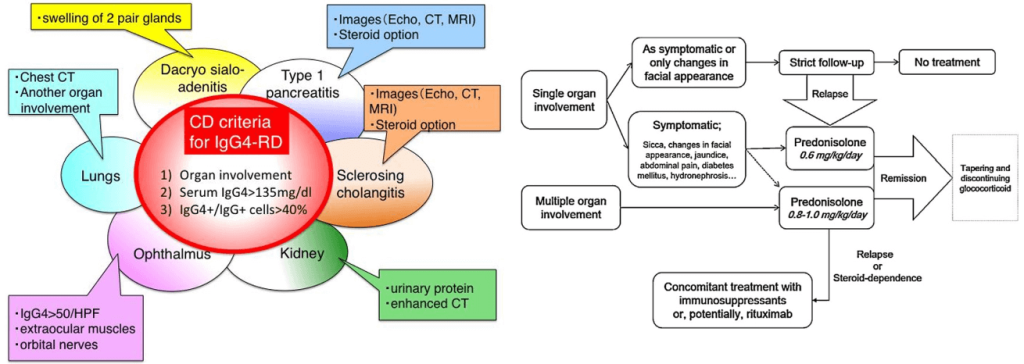
IgG4 related diseases
Bechet’s disease
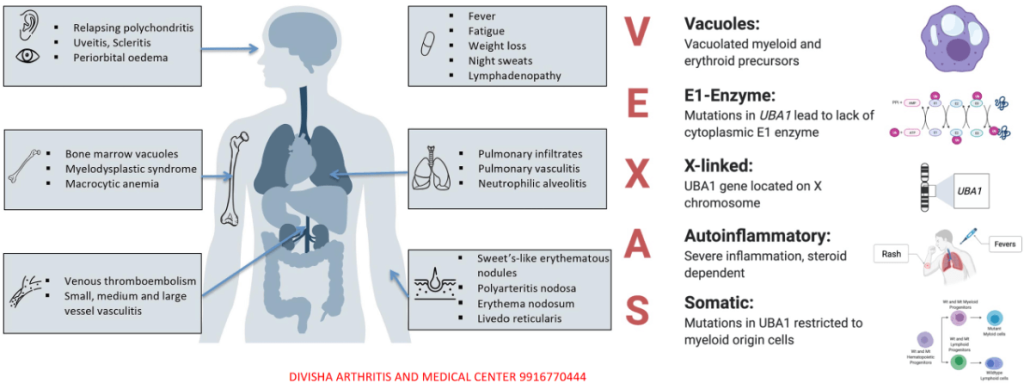
VEXAS syndrome
Always remember this!
History & physical examination very important
| • Focused relevant tests based on history & examination to find out the illness and its severity |
| • Early treatment to mitigate damage |
| • Maintenance treatment & slow taper to prevent relapse |
| • Appropriate diet – low saturated fat, low carbohydrate & absent red meat & no processed food |
| • Physical exercises – cardio, stretching and strengthening exercises daily to improve stamina, energy, muscle balance & self-immunity |
| • Confidence, positive mental strength & belief in self and belief in treatment |
Further Readings:
- Cheema KS, Bit Mansour A, Raychaudhuri SP. What’s new on the horizon for rheumatoid arthritis management. Best Pract Res Clin Rheumatol. 2025 Feb 11:102038. doi: 10.1016/j.berh.2025.102038. Epub ahead of print. PMID: 39939220.
- Ahn EY, So MW. The pathogenesis of gout. J Rheum Dis. 2025 Jan 1;32(1):8-16. doi: 10.4078/jrd.2024.0054. Epub 2024 Nov 6. PMID: 39712248; PMCID: PMC11659655.
- https://vasculitis.org/
- https://www.icd10data.com/ICD10CM/Codes/M00-M99/M30-M36/M35-/M35.2
- Lavalle, S.; Caruso, S.; Foti, R.; Gagliano, C.; Cocuzza, S.; La Via, L.; Parisi, F.M.; Calvo-Henriquez, C.; Maniaci, A. Behçet’s Disease, Pathogenesis, Clinical Features, and Treatment Approaches: A Comprehensive Review. Medicina 2024, 60, 562. https://doi.org/10.3390/medicina60040562
- Alqatari, S.; Alqunais, A.A.; Alali, S.M.; Alharbi, M.A.; Hasan, M.; Al Shubbar, M.D. VEXAS Syndrome: A Comprehensive Review of Current Therapeutic Strategies and Emerging Treatments. J. Clin. Med. 2024, 13, 6970. https://doi.org/10.3390/jcm13226970
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Highly informative