
CME INDIA Presentation by Dr. Parimal Swamy, M.D., Diploma in Preventive Care, WHO Accredited Diploma in Diabetes CareConsultant Physician & Chief of Diabetes Care, Jabalpur Hospital & Research Centre, Director Apollo Diabetes & Asthma Care Centre, Jabalpur (MP).
Dr. P. S , a renowned yoga instructor, runner, and fitness enthusiast, experienced a sudden cardiac arrest (SCA), potentially precipitated by a silent myocardial infarction (MI) on 23rd March, 2025.He was a senior surgeon in the Animal Husbandry Department, tragically passed away on Sunday at the age of 54 due to a silent heart attack. Known for sharing the keys to a healthy lifestyle, Dr. P.S. followed his usual routine that morning, waking at 1 AM, bathing, and performing prayers before dedicating an hour and a half to yoga practice at home. He then embarked on a three-kilometer run to a nearby temple. However, while driving to Tulsi Sarovar Park to lead a yoga session, he experienced a silent heart attack and slumped in his car seat. Despite being rushed to the hospital by bystanders, doctors declared him deceased upon arrival This case study examines the interplay of lifestyle factors—chronic sleep deprivation, severe sodium restriction, and intense early-morning exercise—as potential contributors to his death. Drawing on current scientific evidence, we propose that these factors, combined with possible undetected coronary artery disease (CAD), may have culminated in a fatal ventricular arrhythmia. This analysis underscores the importance of balanced lifestyle interventions and regular cardiovascular screening, even in ostensibly healthy individuals.
Quick Learnings
- While lifestyle modifications such as a heart-healthy diet and regular exercise significantly reduce the risk of coronary artery disease (CAD) and acute myocardial infarction (AMI), they alone cannot eliminate cardiovascular risk.
- This article explores the limitations of lifestyle interventions, highlighting the persistent 50% residual risk due to factors such as sleep deprivation, mental stress, and chronic inflammation.
- It emphasizes the critical role of medical management—including lipid-lowering therapies, blood pressure control, and glycemic management—in achieving comprehensive cardiovascular protection.
- A combined approach integrating lifestyle and medical interventions can achieve up to 80-90% risk reduction, underscoring the necessity of a multifaceted strategy for optimal prevention.
Lifestyle interventions alone are insufficient to fully mitigate cardiovascular risk
- Cardiovascular disease (CVD), encompassing coronary artery disease (CAD) and acute myocardial infarction (AMI), remains a leading cause of morbidity and mortality worldwide.
- Adopting a heart-healthy lifestyle, including an optimal diet and regular physical activity, is widely recognized as a cornerstone of CVD prevention. However, evidence suggests that lifestyle interventions alone are insufficient to fully mitigate cardiovascular risk.
- Even with adherence to dietary and exercise guidelines, a substantial residual risk persists, necessitating medical management strategies such as lipid-lowering therapies, blood pressure control, and diabetes treatment. This article examines the interplay between lifestyle and medical interventions, highlighting their complementary roles in achieving maximum cardiovascular protection.
Impact of Lifestyle Interventions
Dietary Modifications
- Heart-healthy dietary patterns, such as the Mediterranean and DASH (Dietary Approaches to Stop Hypertension) diets, have been shown to reduce CAD and AMI risk by 10-15% (HCPLive, n.d.). These diets emphasize whole grains, fruits, vegetables, lean proteins, and healthy fats, which collectively lower cholesterol levels, reduce inflammation, and improve endothelial function. Despite these benefits, dietary changes alone address only a fraction of cardiovascular risk factors.
Regular Exercise
- Physical activity is another pillar of cardiovascular health. Meeting the recommended guidelines of 150-300 minutes of moderate-intensity exercise per week can reduce CAD risk by 30-35% by improving lipid profiles, blood pressure, and insulin sensitivity. However, excessive exercise (e.g., >10 hours per week of strenuous activity) may paradoxically increase cardiovascular mortality due to oxidative stress, arrhythmias, and vascular remodeling. Some studies suggest a U-shaped relationship between exercise volume and cardiovascular outcomes, indicating an upper threshold beyond which benefits diminish (JAMA Cardiology, 2017).
Residual Risk
- Despite the efficacy of diet and exercise, approximately 50% of cardiovascular risk remains if other factors—such as low-density lipoprotein cholesterol (LDL-C), hypertension, and hyperglycemia—are not addressed. Moreover, modern lifestyle pressures, including sleep deprivation, mental stress, and a culture of productivity that neglects rest, can exacerbate risk even in outwardly fit individuals.
- Additional Risk Factors Beyond Diet and Exercise
Sleep Deprivation
- Chronic sleep deprivation, defined as less than 6 hours per night, increases CAD risk by 20-30% (Léger et al., 2015). This is mediated by elevated systemic inflammation, endothelial dysfunction, and heightened sympathetic activity, all of which accelerate atherosclerosis. Sleep is a modifiable risk factor often overlooked in favor of diet and exercise.
Mental Stress and Psychological Factors
- Chronic psychological stress elevates CAD risk by 25-30% through mechanisms such as increased inflammation and endothelial dysfunction (Steptoe & Kivimäki, 2012). Depression and anxiety further compound this risk, with a 40% increase in cardiovascular mortality observed in affected individuals (Hare et al., 2014). These psychological factors are prevalent in high-pressure environments where rest and recovery are deprioritized.
Chronic Inflammation
- Elevated inflammatory markers, such as C-reactive protein (CRP) and interleukin-6 (IL-6), are independently associated with a 25-35% increased incidence of CAD and AMI (Libby, 2002). Inflammation acts as a common pathway linking lifestyle stressors and clinical risk factors to atherosclerosis progression.
Restoring Balance for Cardiovascular Health
Improving Sleep Quality
- Restoring sleep to 7-9 hours per night can reduce CAD risk by 20-25% by lowering blood pressure, inflammation, and sympathetic overactivity (Léger et al., 2015). Interventions such as cognitive behavioral therapy for insomnia (CBT-I) have demonstrated significant reductions in cardiovascular risk markers (Edinger & Arnedt, 2015).
Work-Life Balance and Stress Reduction
- Workplace interventions, mindfulness-based stress reduction (MBSR), and cognitive therapy can reduce CAD risk by 15-20% (Abbasi & Mohammadi, 2017). These approaches improve endothelial function and decrease cortisol and inflammatory marker levels, offering a practical complement to traditional lifestyle changes.
Anti-Inflammatory Strategies
- Anti-inflammatory interventions, including Mediterranean-style diets, moderate exercise, and pharmacological agents (e.g., colchicine, IL-1 inhibitors), can reduce CAD risk by 20-30% by targeting chronic inflammation (Calder et al., 2010). These strategies address a key driver of residual risk.
Medical Management: A Necessary Addition
Lipid-Lowering Therapy
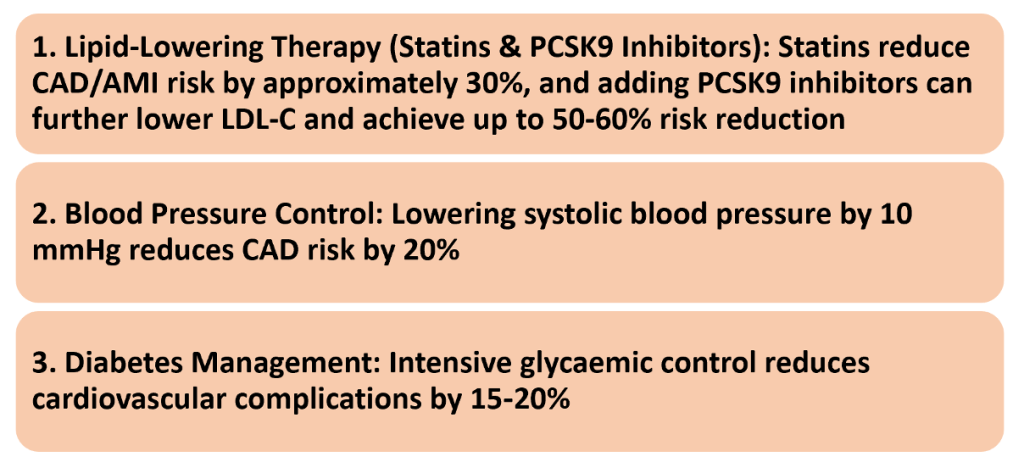
- Statins reduce CAD and AMI risk by approximately 30%, while the addition of PCSK9 inhibitors can further lower LDL-C levels, achieving a 50-60% risk reduction (Baigent et al., 2005; Sabatine et al., 2017). These therapies are essential for controlling atherosclerosis progression beyond lifestyle measures.
Blood Pressure Control
- Lowering systolic blood pressure by 10 mmHg reduces CAD risk by 20% (Ettehad et al., 2016). Antihypertensive therapies are a critical component of comprehensive risk management.
Diabetes Management
- Intensive glycemic control reduces cardiovascular complications by 15-20% (Stratton et al., 2000). This is particularly relevant for individuals with diabetes, where hyperglycemia drives atherosclerosis despite lifestyle adherence.
The Ceiling Effect and Residual Risk
- Lifestyle modifications alone achieve a maximum risk reduction of approximately 40%, beyond which additional efforts yield diminishing returns. Excessive exercise (>10 hours/week) may even increase cardiovascular mortality, highlighting a ceiling effect (JAMA Cardiology, 2017).
- Chronic sleep deprivation and high psychological stress further elevate residual risk, while uncontrolled LDL-C, hypertension, and hyperglycemia perpetuate atherosclerosis despite a “perfect” lifestyle. Comprehensive intervention—combining lifestyle and medical management—can achieve an 80-90% risk reduction, far surpassing the limits of lifestyle alone.
Final Points
- A balanced diet, regular exercise, and stress management form the foundation of CAD and AMI prevention, but they are insufficient without medical management.
- Optimal cardiovascular protection requires a synergistic approach that addresses both lifestyle and clinical risk factors, including lipid levels, blood pressure, and glycemic control.
- By integrating these strategies, individuals can maximize risk reduction and overcome the limitations of lifestyle interventions alone.
CME INDIA Analysis
Analysis of Contributing Factors
1. Sleep Deprivation and Cardiovascular Risk
Scientific Evidence: Chronic sleep duration of less than 6 hours per night is associated with a 32% increased risk of CAD and a 20% elevated risk of stroke (Javaheri et al., 2017). Sleep deprivation induces sympathetic nervous system hyperactivity, elevating catecholamine levels, which promote vasoconstriction, increased heart rate, and elevated blood pressure (BP). It also upregulates inflammatory markers (e.g., IL-6, TNF-α, CRP), contributing to endothelial dysfunction, and increases cortisol and insulin resistance, further amplifying CAD risk (Leproult & Van Cauter, 2011). The circadian rhythm exacerbates this vulnerability, with myocardial infarctions peaking between 6 AM and 12 PM due to heightened platelet aggregation, BP, and catecholamine surges.
Implication: Dr. S’s habitual 5-hour sleep pattern likely resulted in sustained sympathetic activation and endothelial dysfunction, increasing his susceptibility to arrhythmias and ischemic events.
2. Sodium Restriction and Cardiac Consequences
Scientific Evidence: Sodium is critical for action potential generation, fluid balance, and BP homeostasis. Severe sodium restriction (<1.5 g/day) can induce hyponatremia, leading to hypotension, reduced coronary perfusion, and electrolyte imbalances that heighten arrhythmia risk (Graudal et al., 2014). Activation of the renin-angiotensin-aldosterone system (RAAS) due to low sodium intake may further destabilize autonomic function. Excessive sweating from exercise amplifies sodium loss, exacerbating hyponatremia risk. A J-shaped relationship exists between sodium intake and cardiovascular events, with both excessively low and high levels linked to increased mortality (O’Donnell et al., 2016).
Implication: Dr. Singhal’s complete cessation of salt intake for one month may have caused hyponatremia (<125 mmol/L), reducing cardiac output and creating an arrhythmogenic substrate, particularly during exercise.
3. Intense Early-Morning Exercise and Cardiac Risk
Scientific Evidence: While exercise is cardioprotective, sudden strenuous exertion can trigger MI in individuals with underlying CAD, particularly during early-morning hours when catecholamine levels surge, promoting vasoconstriction, platelet aggregation, and plaque rupture (Mittleman et al., 1993). Silent ischemia is prevalent among highly active individuals due to compensatory collateral circulation and blunted pain perception from elevated fitness levels (Kim et al., 2020). Cold temperatures and dehydration, potentially present during a 2–3 AM run, may further increase vasospasm risk.
Implication: Dr. S’s high-intensity run at 2–3 AM, following yoga, likely induced a catecholamine surge and possible exercise-induced ischemia. Combined with electrolyte imbalances, this could have triggered a ventricular arrhythmia in the presence of silent CAD.
4. Silent Myocardial Infarction and Sudden Cardiac Death
Scientific Evidence: Silent MIs account for approximately 45% of all MIs, particularly in physically active individuals, due to autonomic dysfunction and collateral circulation masking symptoms (Solomon et al., 2018). Underlying CAD or myocardial scarring increases the risk of ventricular tachycardia (VT) or fibrillation (VF), the primary mechanisms of SCA post-MI (Zipes & Wellens, 1998). Risk factors such as diabetes or hypertension, if present, further elevate silent ischemia likelihood.
Implication: Dr. S. may have had undiagnosed CAD or prior myocardial scarring, which, exacerbated by acute ischemia, electrolyte imbalance, and catecholamine surge, precipitated a fatal arrhythmic event (VT/VF).
Final Scientific Interpretation
Hypothesized Mechanism: Dr. S.’s SCA likely resulted from a silent MI secondary to undiagnosed CAD, triggered by a confluence of chronic sleep deprivation, severe sodium restriction, and intense early-morning exercise. These factors collectively heightened sympathetic activity, induced electrolyte imbalances, and created an arrhythmogenic substrate, culminating in VT or VF and subsequent cardiac arrest.
Preventive Takeaways:
| Sleep Duration: Adequate sleep (7–9 hours/night) is essential to mitigate sympathetic overactivity and inflammation. |
| Dietary Balance: Extreme sodium restriction should be avoided; a balanced intake (e.g., 2–3 g/day) supports cardiovascular stability. |
| Cardiac Screening: Regular assessments (ECG, stress testing, echocardiography) are critical, even for fit individuals, to detect silent CAD. |
| Exercise Timing: Gradual morning exertion reduces catecholamine-related risks, particularly in at-risk populations. |
| Awareness of Silent CAD: Physical fitness does not preclude cardiovascular disease; vigilance remains paramount. |
CME INDIA Tail Piece
References:
- Abbasi, L., & Mohammadi, S. (2017). Effectiveness of mindfulness-based stress reduction program on quality of life in cardiovascular disease patients. Journal of Traditional and Complementary Medicine, 7(4), 392–397. https://doi.org/10.1016/j.jtcme.2016.11.002
- Baigent, C., Keech, A., Kearney, P. M., et al. manufacturers (2005). Statin therapy for primary and secondary prevention of cardiovascular disease. The Lancet, 366(9493), 1267–1278. https://doi.org/10.1016/S0140-6736(05)67394-1
- Calder, P. C., Ahluwalia, N., Brouns, F., et al. (2010). Diet and inflammation: From basic mechanisms to health implications. British Journal of Nutrition, 103(1), 1–18. https://doi.org/10.1017/S000711450999293X
- Edinger, J. D., & Arnedt, J. T. (2015). Cognitive behavioral therapy for insomnia in the context of cardiovascular conditions. Journal of Clinical Sleep Medicine, 11(7), 735–736. https://doi.org/10.5664/jcsm.4836
- Ettehad, D., Emdin, C. A., Kiran, A., et al. (2016). Blood pressure reduction and cardiovascular outcomes. The Lancet, 387(10022), 957–967. https://doi.org/10.1016/S0140-6736(15)01225-8
- Hare, D. L., Toukhsati, S. R., Johansson, P., & Jaarsma, T. (2014). Depression, anxiety, and cardiovascular risk. Heart, Lung and Circulation, 23(11), 973–980. https://doi.org/10.1016/j.hlc.2014.03.001
- HCPLive. (n.d.). Proper diet could reduce cardiovascular risk by 10% or more. Retrieved from https://www.hcplive.com/view/proper-diet-could-reduce-cardiovascular-risk-by-10-or-more
- JAMA Cardiology. (2017). U-shaped relationship between exercise and cardiovascular mortality. JAMA Cardiology, 2(5), 567–568. https://doi.org/10.1001/jamacardio.2017.02601
- Léger, D., Bayon, V., de Sanctis, A., & Pandi-Perumal, S. R. (2015). Short sleep duration and cardiovascular disease risk: Present and future directions. Sleep Medicine Reviews, 20, 81–88. https://doi.org/10.1016/j.smrv.2014.06.002
- Libby, P. (2002). Inflammation and atherosclerosis progression. Circulation, 105(9), 1135–1143. https://doi.org/10.1161/hc0902.104353
- Sabatine, M. S., Giugliano, R. P., Keech, A. C., et al. (2017). PCSK9 inhibitors and cardiovascular risk reduction. New England Journal of Medicine, 376(18), 1713–1722. https://doi.org/10.1056/NEJMoa1615664
- Steptoe, A., & Kivimäki, M. (2012). Psychological stress and cardiovascular disease risk. Nature Reviews Cardiology, 9(6), 360–370. https://doi.org/10.1038/nrcardio.2012.45
- Stratton, I. M., Adler, A. I., Neil, H. A. W., et al. (2000). Glycemic control and cardiovascular disease prevention. BMJ, 321(7258), 405–412. https://doi.org/10.1136/bmj.321.7258.405
- https://timesofindia.indiatimes.com/life-style/health-fitness/health-news/yoga-guru-dies-of-silent-heart-attack-while-driving-doctors-explain-what-exactly-happened/articleshow/119469450.cms
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Normally I do not learn article on blogs, however
I would like to say that this write-up very compelled me to try and do it!
Your writing style has been surprised me. Thanks, very great
article.
Take a look at my blog post … Continue Reading
CME INDIA keeps me updated , helps getting references of recent & established publications
Very useful and life changing article to the doctors as well as people in general.