
CME INDIA Presentation by Dr. S. K. Gupta, Delhi, Dr. N. K. Singh, Dhanbad, Dr. Akash N. Singh, Vadodara, Dr. Anuradha Kappor, Mumbai, Dr. Bijay Patni, Kolkata.
Like King Vikramaditya’s endless struggle with the elusive Betaal, India’s battle with COVID-19 seems cyclical—just as the threat appears to fade, a new challenge emerges. In May 2025, India is facing a fresh surge in cases, with states like Kerala, Maharashtra, and Delhi reporting rising numbers. New variants such as NB.1.8.1 and LF.7, now under WHO monitoring, are driving this uptick. Though most cases remain mild, the situation calls for renewed vigilance, echoing Vikram’s tireless pursuit—persistent, alert, and ready for what lies ahead.
Has COVID become Seasonal?
- Since mid-February 2025, global SARS-CoV-2 activity has been increasing.
- Test positivity rate has reached 11% (as of 11 May 2025), comparable to the July 2024 peak (12%).Global figures
- This surge is mainly driven by the Eastern Mediterranean, South-East Asia, and Western Pacific regions.
- Positivity rate has risen from 2% (Feb 2025) to 11% (May 2025).
- But duration and data is still low to label as seasonal disease like influenza.
- No clear seasonal pattern of SARS-CoV-2 established yet.
Variants Surveillance
- Still JN.1 is a major Variant (it is a sub variant of Omicron) under circulation since Jan 2024.
- LP.8.1 (previously globally dominant variant) is declining.
- NB.1.8.1, a Variant Under Monitoring (VUM), is increasing, now accounting for 10.7% of global sequences.
- √NB.1.8.1 is a descendant of XDV.1.5.1 → JN.1.
Key spike mutations in NB.1.8.1:
- T22N, F59S, G184S, A435S, V445H, T478I
- V445H → May increase transmissibility.
- A435S → May modestly reduce neutralization by antibodies.
- T478I → May enhance immune evasion.
NB.1.8.1 is spreading rapidly in many regions, though _only 5 sequences reported from South East Asia(Mid May 2025 figures)
Public Health Implications of NB.1.8.1
- Despite increased circulation, no additional public health risk has been identified for NB.1.8.1 or LP.8.1.
What is special about Sars-Cov-2?
- Virus evolution remains unpredictable.
Vaccination Status (2024 Data)
- Global vaccine uptake among high-risk groups remains low:
- Older adults: Only 1.68% vaccinated in 2024 (75 countries).
- Health & care workers: Only 0.96% vaccinated (54 countries).
- Significant regional and income-based disparities in vaccination coverage. Higher income group still better vaccinated.
WHO Recommendations
- Countries should maintain a risk-based, integrated COVID-19 response.
- High risk group individuals like elderly immunocompromised Advanced DM CKD CoPD, people on steroids better use Masks, keep off gatherings.
- Govt. of India should consider making vaccines available for high risk groups but no vaccine mandate for general public.
- Vaccination remains key to prevent severe disease and deaths, especially for at-risk populations.
India’s COVID-19 Status – May 26, 2025
- Mild Surge Driven by New Omicron Sub-Variants
Source: MoHFW | INSACOG
Current National Snapshot
As of May 28, 2025, India is witnessing a mild uptick in COVID-19 cases, primarily attributed to the emergence of new Omicron sub-lineages NB.1.8.1 and LF.7. Active cases across the country have risen to 1,010, reflecting a mild but steady upward trend in select regions.
States with the Highest Active Caseloads
- Kerala – 430 active cases
- Maharashtra – 209
- Delhi – 104
- Gujarat – 83
- Karnataka – 80 (including 73 in Bengaluru alone)
- These numbers are being closely monitored, though hospitalisation remains low.
Circulating Variants & Clinical Presentation
The predominant strains in circulation—NB.1.8.1 and LF.7—are subvariants of the Omicron lineage. These strains are highly transmissible, but not associated with increased severity or hospitalisation.
Common Symptoms:
- Sore throat
- Fatigue
- Nasal congestion
- Diarrhea
Symptoms are largely self-limiting and resemble a mild upper respiratory viral illness.
Clinical Pearls for Practitioners
- Symptomatic management in OPD settings is adequate for most patients.
- Antiviral therapy (e.g., nirmatrelvir/ritonavir) should be reserved for high-risk groups such as the elderly, immunocompromised individuals, and those with significant comorbidities.
- Clinicians should closely monitor older adults and patients with underlying conditions, even if symptoms appear mild.
- There is no recommendation for lockdowns or movement restrictions at this time. Instead, the focus remains on:
- Vaccination of at-risk populations
- Use of masks in crowded/public indoor spaces
- Strengthened genomic surveillance and timely reporting
Public Health Perspective
Despite the rise in cases, public health officials emphasize that there is no cause for panic. The current variants are behaving in line with previous Omicron waves—spreading efficiently, but not causing significant morbidity or strain on hospital systems.
Important Points
- The new Omicron sub-lineages NB.1.8.1 and LF.7 are highly transmissible but not more virulent.
- Continue to vaccinate vulnerable individuals, encourage basic preventive measures, and stay vigilant, especially in outpatient settings.
- No major disruptions are anticipated at this time, provided preventive strategies are upheld.
Stay informed. Stay protected. Continue clinical vigilance without alarm.
LF.7 COVID-19 Variant – 2025 Update
What is LF.7?
LF.7 is a newly emerging subvariant of Omicron, closely related to NB.1.8.1 and a descendant of the JN.1 lineage. It carries significant mutations in the spike protein, which are associated with an increased potential for transmission. The World Health Organization (WHO) has currently classified LF.7 as a “Variant Under Monitoring,” indicating the need for close observation but not immediate concern regarding severity.
Current Situation in India – May 2025
As of May 2025, India has reported a small number of LF.7 and NB.1.8.1 cases. Specifically, four cases of LF.7 have been confirmed in Gujarat, while a single case of NB.1.8.1 has been detected in Tamil Nadu. Fortunately, most of these cases have been mild and manageable at home, without the need for hospitalisation.
Clinical Presentation – LF.7 Symptoms
The LF.7 subvariant is presenting with symptoms similar to earlier Omicron strains, particularly BA.2. Most patients report cold-like symptoms such as a runny nose, sore throat, fatigue, headache, dry cough, muscle aches, and low-grade fever. These are typically mild and self-limiting in otherwise healthy individuals.
Severity and Risk Factors
So far, there is no evidence to suggest that LF.7 is associated with increased hospitalisation or mortality. However, vulnerable populations—including the elderly, immunocompromised individuals, people with diabetes or cardiovascular disease, and pregnant women—are still advised to follow standard precautions.
Recommended Precautions (Still Relevant in 2025)
Despite the mild nature of current cases, standard COVID-19 precautions remain important:
- Stay up to date with vaccination and booster doses to prevent severe illness.
- Wear masks in crowded or enclosed public spaces.
- Maintain proper hand hygiene using sanitizers or soap.
- Practice physical distancing, especially in poorly ventilated areas.
- Isolate and get tested if symptomatic.
Treatment Protocols
Most LF.7 infections can be managed with supportive care, including rest, hydration, and paracetamol. Antiviral medications or corticosteroids should only be used in severe cases, in accordance with the Ministry of Health and Family Welfare (MoHFW) guidelines. High-risk individuals, particularly the elderly and those with diabetes, should have their vital signs—especially oxygen saturation (SpO₂)—monitored regularly.
Public Health Response and Surveillance
INSACOG continues to maintain heightened genomic surveillance across the country. Hospitals have been advised to prepare for any potential increase in cases by ensuring adequate supplies of ventilators, oxygen cylinders, and trained staff.
Key Takeaways for Clinicians Healthcare professionals are urged not to panic but to stay informed as the situation evolves. LF.7 appears to be a mild variant that can be managed similarly to seasonal viral infections. Clinicians should continue to promote vaccination, appropriate masking, and timely reporting of suspected cases to health authorities.
COVID-19 Vaccines and Immune System Health: Should We Be Concerned About Mixing Vaccine Types?
Asked By Dr. Pradipta Mahapatra
As we move into the fifth year of the COVID-19 pandemic, questions continue to emerge about the long-term effects of vaccination. A frequently asked question, posed by Dr. Pradipta Mahapatra, is:
“If someone has received a protein, subunit, mRNA, or inactivated COVID-19 vaccine, could receiving a different type of vaccine later cause problems with their immune system? Who can definitively answer this?”
What the Evidence Says:
As of now, no credible evidence suggests that receiving different types of COVID-19 vaccines—whether protein subunit (e.g., Novavax), mRNA (e.g., Pfizer, Moderna), or inactivated/killed virus vaccines (e.g., Sinovac, Covaxin)—poses a long-term risk to the immune system.
All of these vaccines work by training the immune system to recognize components of the SARS-CoV-2 virus, most commonly the spike protein. The goal is to create immunological memory so that the body can respond rapidly and effectively if exposed to the virus again.
Mixing Vaccines: Is It Safe?
Mixing vaccine platforms—also known as heterologous boosting—has been the subject of numerous studies worldwide. Research published in peer-reviewed journals, including The Lancet (2021–2022), has shown that mixing vaccine types can often enhance the immune response, particularly in terms of producing broader antibody and T-cell activity.
In fact, heterologous combinations, such as giving an mRNA booster after an inactivated or adenoviral vector vaccine, have shown strong immunogenicity and favorable safety profiles in most populations.
Side Effects and Long-Term Considerations
Mild side effects like fatigue, fever, or localized soreness are common across all vaccine types and are generally self-limiting. These occur whether vaccines are administered in homologous (same type) or heterologous (different type) regimens.
Rare adverse events, such as Myocarditis (mostly associated with mRNA vaccines), and Thrombosis with thrombocytopenia syndrome (TTS) (linked to certain adenoviral vector vaccines), have been documented. However, these are not indicative of broader immune dysfunction, nor are they associated with mixing vaccine types.
Importantly, the immune system is built to handle repeated and varied antigen exposures—a fundamental principle underlying immunology and vaccine development. That said, long-term effects beyond 3–4 years post-vaccination are still being monitored, as COVID-19 vaccines are relatively new. Continued global surveillance and long-term cohort studies are critical in this regard.
Conclusion
At present, mixing different COVID-19 vaccine types does not appear to compromise immune system health. On the contrary, such strategies may offer broader protection in the evolving viral landscape. While cautious monitoring remains essential, there is no cause for alarm based on current scientific evidence. As clinicians, we must rely on data, not fear, and continue to educate our patients accordingly.
Understanding the Science Behind Mixing Vaccine Types (Heterologous Boosting) As the fight against COVID-19 continues, vaccine strategies have evolved beyond primary immunization. One of the most promising approaches is heterologous boosting—commonly known as the “mix-and-match” method—where a booster dose is given using a different vaccine platform from the one used in the initial series.
What is Heterologous Boosting?
Unlike homologous boosting, where the same vaccine is used for all doses, heterologous boosting involves combining different types of vaccines—such as using an mRNA vaccine after an inactivated or protein-based primary series. This approach is backed by robust scientific evidence, demonstrating both safety and enhanced immunogenicity.
Key Findings from Global and Indian Studies
- Stronger and Broader Immune Response: Heterologous boosters have been shown to induce a more robust and durable immune response—both humoral (antibody-mediated) and cellular (T-cell)—compared to homologous boosters.
- Superiority of mRNA Boosters: When mRNA vaccines are administered as boosters after a primary course with inactivated or protein-based vaccines, they lead to a significant increase in antibody titers and T-cell activation.
- Indian Data Supports Efficacy and Safety: Recent Indian studies, including those evaluating intranasal adenoviral vector vaccines administered after Covaxin or Covishield, confirm that heterologous regimens are safe and elicit strong immune responses.
- Long-lasting Immunity: One-year follow-up data reveals that heterologous booster regimens sustain higher IgG antibody levels, contributing to prolonged humoral immunity—even in individuals with prior natural infection.
Clinical Implications
- No Immune Harm: There is no evidence that mixing vaccine types harms the immune system or causes long-term immune dysfunction.
- Enhanced Protection Against Variants: Heterologous strategies are particularly valuable in the context of emerging variants, helping broaden and strengthen overall immunity.
- Real-world Challenge: Despite its promise, the main barrier is availability—many vaccine platforms are currently unavailable in the open market in India, limiting widespread implementation.
Conclusion
Heterologous boosting has emerged as a scientifically validated and safe strategy for improving vaccine-induced protection. While logistical hurdles remain, especially in the Indian context, ongoing research and regulatory support may help pave the way for broader adoption of this effective approach to pandemic control.
Which COVID-19 Vaccine Should You Choose in 2025?
Asks Dr. Aparna Bhaumik, Kolkata
As we move through 2025, the landscape of COVID-19 vaccination continues to evolve. With new variants and shifting public health priorities, the question on everyone’s mind remains: Which vaccine is best suited for current needs, especially as a booster?
A concise guide to the recommended and available COVID-19 vaccines in India and globally as of May 2025, particularly relevant for boosters and high-risk individuals.
Recommended COVID-19 Vaccines (India & Global)
- Covovax (Serum Institute, Novavax-based)
- Type: Protein subunit vaccine
- Use: Approved for booster doses in India
- Effectiveness: Demonstrated protection against Omicron sub-lineages
- CorBEvax (Biological E)
- Type: Recombinant protein vaccine
- Use: Approved for heterologous booster doses
- Profile: Excellent safety data, especially in elderly and comorbid populations
- Covaxin (Bharat Biotech)
- Type: Whole inactivated virus vaccine
- Use: Primary series and limited use as booster
- Limitation: Reduced neutralization capacity against newer Omicron variants
- mRNA Vaccines (Pfizer-BioNTech / Moderna)
- Availability: Private/imported route in India
- Effectiveness: Strong protection against current Omicron subvariants
- Use Case: Ideal for immunocompromised individuals and international travelers
- Updated Variant-Specific mRNA Boosters
- Status: Not yet approved in India, but in use in US, UK, EU
- Target: XBB.1.5, JN.1, and newer Omicron lineages
- Deployment: Key part of global booster campaigns (2023–2025)
Booster Guidance (ICMR & WHO – Q1–Q2 2025)
- High-risk groups (age >60, comorbidities, immunocompromised): Annual booster recommended
- General population (healthy individuals under 50): No mandatory boosters at present
- Pregnant women & healthcare workers: Annual booster advisable, especially in high-exposure settings
Clinical Pearl from CME INDIA
In 2025, Covovax and CorBEvax remain the most accessible and effective booster choices within India.
For those who are immunocompromised or need international protection, mRNA vaccines—if accessible—offer the broadest defense against evolving subvariants.
As always, vaccine choice should be tailored to individual risk factors, exposure, and availability. Stay updated through official health channels and consult your physician for personalized recommendations.
CME INDIA Booster Dose Recommendations – May 2025
As the COVID-19 pandemic transitions into an endemic phase, vaccination strategies are being recalibrated based on evolving evidence, variant dynamics, and population risk profiles. Here’s a clear and concise overview of the latest booster dose guidance as of May 2025:
General Population (<50 years, Healthy Individuals)
- Current Recommendation: No booster doses are mandated or routinely recommended for healthy adults under 50 years of age.
- Rationale: With declining severe disease rates and widespread baseline immunity, additional booster doses offer minimal incremental benefit in this group at present.
High-Risk Groups (Elderly, Comorbid, Immunosuppressed)
- Recommendation: Annual booster may be considered, especially if more than 12 months have passed since the last dose.
- Note: This is not a blanket recommendation; decisions should be individualized based on exposure risk, immune status, and medical history.
- Vaccine Consideration: Updated monovalent vaccines targeting circulating Omicron subvariants (such as JN.1, LF.7, NB.1.8) are anticipated to provide better variant-specific protection. However, these updated formulations are not yet widely available in India.
Pregnant Women & Healthcare Workers
- Guidance: One annual booster dose may be considered, particularly for those with high risk of exposure or underlying health vulnerabilities.
- Why It Matters: Protection of frontline workers and vulnerable maternal populations remains a public health priority, especially during seasonal surges.
Summary
- Healthy <50 years – Not recommended currently
- Elderly/Comorbid/Immunosuppressed – Consider annual booster if >12 months since last dose
- Pregnant Women & HCWs – Consider annual booster in high-risk settings
CME INDIA Insight:
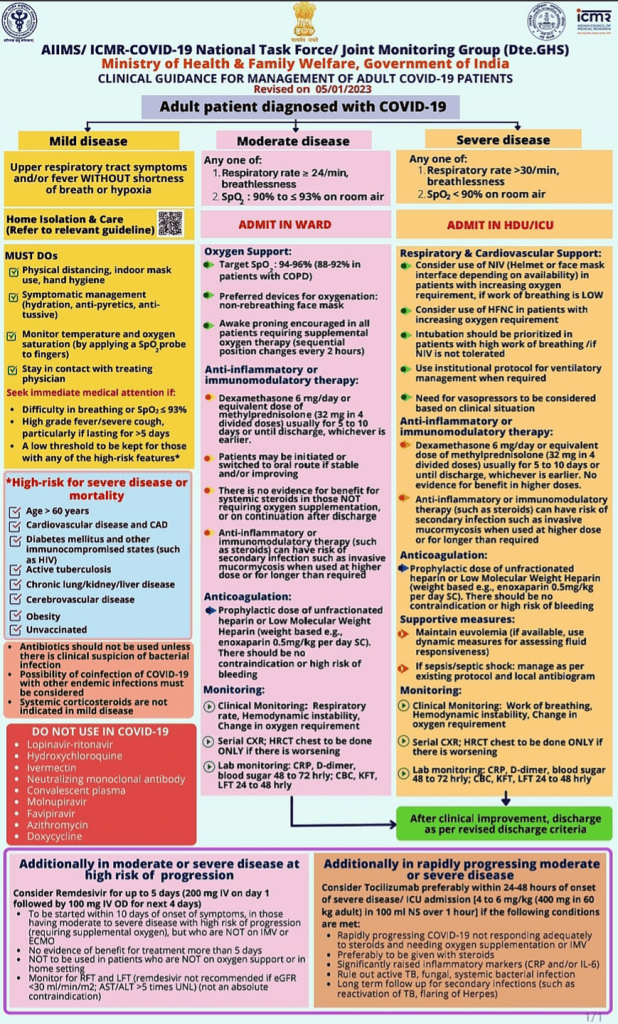
Stay informed through national and state guidelines. Booster decisions should balance current exposure risk, vaccine availability, and individual clinical context. Following PIC is the present treatment Protocol too:
CME INDIA Tail Piece
By Dr. S. K. Gupta
- Surge is seasonal and predominantly by JN.1 and B.2 sub variants.
- Some media houses have reported surge by NB.1.8.1 and LF.7 for which only sporadic cases have been found.
- Vaccines are not available as Covishield production stopped way back in 2022.
- Bhart Biotech is not reporting any data.
- Corbevax by Biological E is also not available.
- Cowin app though active but fails to book any appointment.
- Vaccine mandate was declared unconstitutional by Supreme Court after the pandemic.
References:
- INSACOG Update, May 2025
- WHO Variant Tracker, May 2025
- JAMA: Global Variant Surveillance (2024–2025)
- MoHFW Advisory, India, May 2025, https://covid19dashboard.mohfw.gov.in/
- http://covid19dashboard.mohfw.gov.in
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Very nicely explained