
CME INDIA Presentation by Dr. Vaibhav Agnihotri, MBBS, DCH, DNB (Pediatrics), Fellowship in Neonatology, Fellowship in Allergy, Asthma & Immunology (PGI, Chandigarh), PGPN (Boston University), PCBD (Johns Hopkins, USA), MAIP, MANBD, Pediatrician | Allergy Specialist | Neonatologist, Head – Pediatrics & Neonatology | Medical Superintendent – Soni Hospital, Jaipur,NABH Assessor | National Trainer (PALS & NRP).
Based on a presentation at CID-2025, Mumbai, 6th August.
Did We Treat… or Make It Worse?
Up to 40% of people with diabetes report allergic symptoms – yet allergies remain among the most under-recognized comorbidities.
A Prevalnce Paradox
- A scoping review reported that the prevalence of asthma in individuals with Type 1 diabetes (T1DM) varied widely, ranging from 1.7% to 23.1%.
- Allergic rhinitis appears less common among people with hyperglycemia or metabolic syndrome, with an estimated odds ratio of ~0.8 for rhinitis in the presence of high blood sugar.
- Autoimmune conditions such as T1DM are linked to a higher risk of chronic urticaria; one study found the odds of urticaria to be ~7.7 times greater in patients with diabetes.
- In contrast, findings from a large Danish cohort showed no significant differences in the prevalence of atopic dermatitis, allergic rhinitis, or asthma between children with T1DM and healthy controls.
TH1/TH2 Paradigm
- Allergic Diseases (Asthma, Atopic Dermatitis, etc.):
- Driven predominantly by Th2 cell responses.
- Key cytokines: IL-4, IL-5, IL-13.
- Promote IgE production, activate mast cells and eosinophils, leading to the hallmark allergic inflammation.
- Type 1 Diabetes Mellitus (T1DM):
- A classic Th1-mediated autoimmune disorder.
- Th1 cells and cytokines such as IFN-γ drive destruction of pancreatic β-cells.
- This Th1-dominant response was traditionally believed to counterbalance or suppress Th2-driven allergic responses.
“Inverse Relationship – Does It Really Exist?”
- Clinical Evidence: Contrary to the traditional view, several studies show similar or even higher prevalence of asthma and allergic sensitization in patients with T1DM compared to controls.
- Genetic & Environmental Factors: Infections, microbial exposure, and other environmental triggers strongly influence the immune balance between Th1 and Th2.
- Beyond Th1/Th2: The discovery of Th17 cells and recognition of immune cell plasticity complicate the simple “Th1 vs Th2” model.
- Regulatory T Cells (Tregs): Dysfunctional Treg activity may fail to suppress both Th1 and Th2 pathways, allowing coexistence of autoimmunity and allergy.
- Local Immune Niches: Even under a systemic Th1-dominant profile (as in T1DM), localized Th2-driven inflammation at specific tissues can still drive allergic manifestations.
Unhealed Heat:
Chronic Inflammation Fans Allergic Flames
- Pro-inflammatory Metabolism:
- Type 2 Diabetes (T2DM) and obesity create a chronic low-grade inflammatory state, marked by elevated cytokines such as IL-6 and TNF-α.
- This milieu can exacerbate asthma and promote airway hyperreactivity.
- Allergy–Metabolism Crosstalk:
- Severe allergic diseases (e.g., asthma) can in turn amplify systemic inflammation.
- This feedback loop contributes to worsening insulin resistance and metabolic imbalance.
Guardians Gone Rogue: Autoimmunity
- Autoimmune Overlap: People with Type 1 Diabetes (T1DM) frequently develop other autoimmune conditions such as autoimmune thyroid disease, celiac disease, and vitiligo.
- Shared Immune Predisposition: This reflects an underlying immune dysregulation, where the body’s “guardians” (immune cells) mistakenly attack self-tissues instead of protecting them.
- Broader Impact: Such immune misfiring may also manifest as other autoimmune-mediated disorders, emphasizing the need for holistic surveillance in T1DM patients.
| Common Allergic Conditions in Diabetes |
| Allergic Rhinitis |
| Asthma |
| Chronic Urticaria |
| Insulin Allergy |
| Adhesive/Device Allergy (e.g., pumps, sensors) |
Case 1
A 58-year-old female with Type 2 Diabetes Mellitus presents with persistent sneezing, watery rhinorrhea, and nasal congestion.
- HbA1c: 8.1%
- Current meds: Metformin, Glimepiride
Question: What would be your initial treatment choice?
Options:
A) Prednisolone 20 mg PO
B) Cetirizine 10 mg + Fluticasone nasal spray
C) Diphenhydramine at night
D) Montelukast only
Correct Answer: B) Cetirizine 10 mg + Fluticasone nasal spray
Explanation:
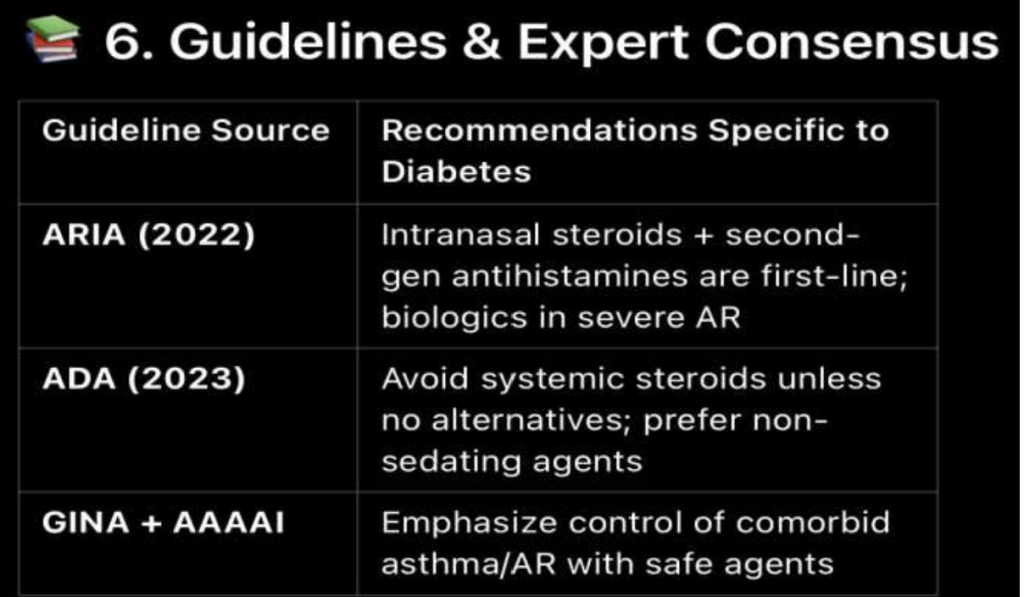
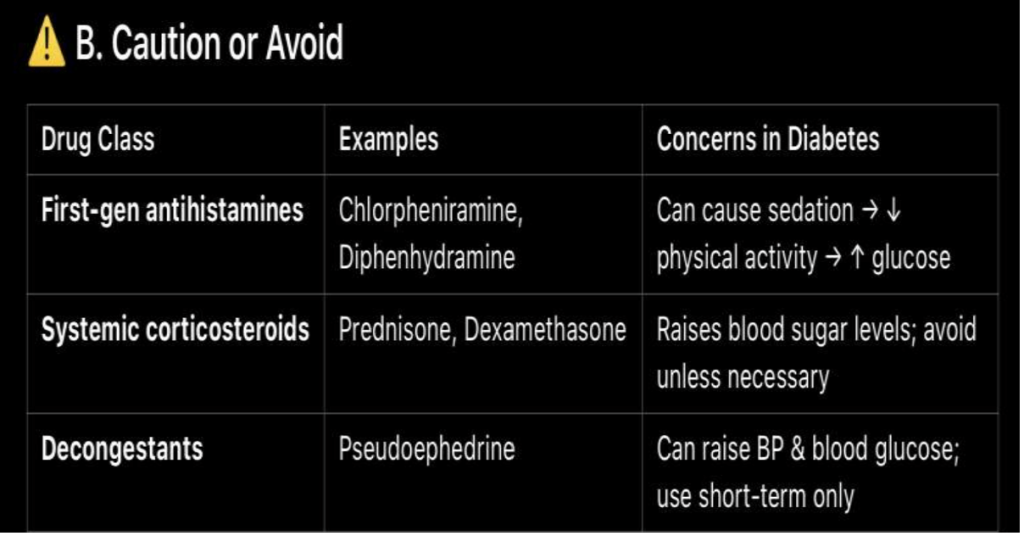
- Prednisolone (A): Systemic steroids are not recommended as first-line therapy for allergic rhinitis due to adverse effects (especially in diabetes where steroids worsen glycemia).
- Cetirizine + Fluticasone (B): Combination of a non-sedating antihistamine with an intranasal corticosteroid is the gold standard first-line therapy for moderate–severe allergic rhinitis. Safe, effective, and evidence-based.
- Diphenhydramine (C): First-generation antihistamine; causes sedation, anticholinergic effects, not preferred in elderly/diabetics.
- Montelukast only (D): Leukotriene receptor antagonists may help but are less effective than intranasal steroids and usually reserved for add-on therapy.
Clinical Pearl: In diabetic patients with allergic rhinitis, always prefer topical (intranasal) steroids over systemic to avoid worsening metabolic control
Sweet and Sneeze – Allergic Rhinitis (AR) in Diabetes
- Prevalence:
- General population: ~10–30%
- Diabetic patients: ~5–15% (slightly lower in some studies)
- Evidence:
- Korean NHANES (2013): Lower prevalence of AR in diabetes, possibly linked to immune dysregulation.
- Italian cohort (2021): Mildly increased AR symptoms in uncontrolled diabetes, driven by systemic inflammation.
- Pathophysiological Links:
- Innate immunity impairment in diabetes alters defense against allergens.
- Chronic hyperglycemia → low-grade systemic inflammation → mucosal hypersensitivity.
- Reduced epithelial barrier → greater allergen penetration.
- Th1/Th2 imbalance:
- Early diabetes (Th1-dominant) may suppress AR.
- Poorly controlled diabetes shifts balance → increased AR risk.
A. Preferred Medications (Minimal Glycemic Impact)
| Drug Class | Examples | Glycemic Impact | Comments |
| Second-generation antihistamines | Cetirizine, Loratadine, Fexofenadine | None | Safe, non-sedating, no effect on glucose levels |
| Intranasal corticosteroids | Fluticasone, Mometasone | Minimal (topical use) | Preferred for persistent symptoms, very low systemic absorption |
| Leukotriene receptor antagonists | Montelukast | None | Good for patients with asthma + AR; no effect on blood sugar |
| Nasal saline sprays | — | — | Adjunct therapy, completely safe |
Sweet and Sneeze – AR in Diabetics
Sweet and Sneeze – AR in Diabetics
Practical Management Algorithm
| Diagnosis confirmation – via history ± SPT |
| Start 2nd-gen antihistamine (e.g., loratadine) |
| Add intranasal steroid if persistent (e.g., fluticasone) |
| If uncontrolled or polysensitized – start immunotherapy |
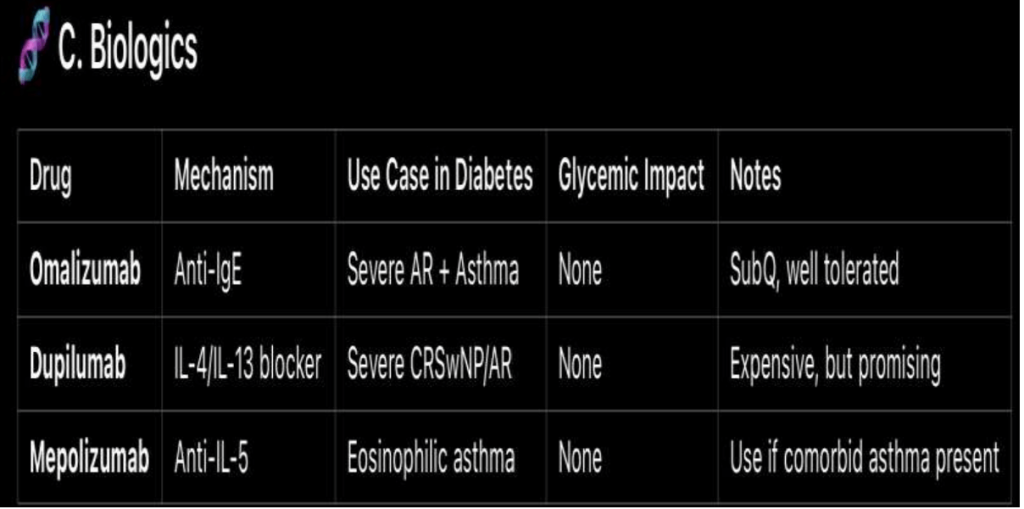
| Severe or refractory? → Consider biologics (Omalizumab) |
Case
A 54-year-old man with Type 2 Diabetes (HbA1c 7.8%) and moderate persistent asthma reports:
- Frequent nocturnal symptoms
- Uses salbutamol 3–4 times/week
- On budesonide 400 mcg BID
Question: What is the most appropriate next step in managing his asthma while ensuring optimal glycemic control?
Options:
A. Increase budesonide dose to 800 mcg BID
B. Start oral prednisolone 20 mg/day for 2 weeks
C. Add long-acting beta agonist (formoterol) to current ICS
D. Switch to mepolizumab (biologic)
Correct Answer: C. Add long-acting beta agonist (formoterol) to current ICS
Explanation:
- A. Increase budesonide to 800 mcg BID: High-dose ICS increases risk of systemic steroid effects, including worsening glycemic control in T2DM. Step-up by dose escalation is not first choice when patient is already symptomatic on medium-dose ICS.
- B. Oral prednisolone: Short courses may help in acute exacerbations, but oral steroids significantly worsen blood sugar control and are not recommended as a step-up for persistent asthma symptoms.
- C. Add LABA (formoterol): Guideline-recommended step-up therapy (GINA). Adding a LABA to an ICS is more effective than doubling ICS dose, improves symptom control, reduces exacerbations, and avoids systemic steroid burden—ideal for a diabetic patient.
- D. Biologic (mepolizumab): Reserved for severe eosinophilic asthma not controlled on high-dose ICS + LABA. Not appropriate at this stage.
Clinical Pearl: In diabetic patients with asthma, avoid unnecessary systemic steroids; prefer ICS + LABA combinations for step-up therapy to balance asthma control with glycemic safety.
Breathless and Sweet – Navigating Asthma in Diabetes
- Asthma Prevalence:
- General population: ~8–10%
- In T2DM: 14–19% (≈2× higher)
- Women with diabetes have a higher risk than men
- Why More Common?
- Chronic low-grade inflammation in diabetes contributes to airway hyperreactivity
- Diabetes & Asthma Control – The Interplay:
- Steroid therapy → raises blood glucose
- Systemic inflammation → worsens both asthma and diabetes
- Insulin resistance → alters airway reactivity
- Obesity → common link, aggravates outcomes
Diagnosis Strategy – Asthma in Diabetics
- History & Symptoms – wheeze, cough, nocturnal symptoms, triggers
- Objective Testing – peak flow monitoring / spirometry with reversibility check
- Glycemic Status – assess recent blood sugar fluctuations / HbA1c
- Medication Review – look for overuse of SABA or inappropriate steroid use
- Allergic/Eosinophilic Profile – consider eosinophil count / IgE when evaluating for biologic therapy
- Comorbidity Screening – obesity and GERD are common and worsen both asthma and diabetes
Asthma Management in Diabetics – Stepwise Strategy
| Step | Preferred Strategy | Remarks |
| Mild Asthma | Inhaled corticosteroids (ICS) + LABA or LTRA | Prefer low-dose ICS, use spacer to reduce systemic absorption |
| Moderate | ICS–LABA combo | Prefer budesonide–formoterol due to lower systemic effects |
| Severe | Add-on therapy like LTRA (e.g., montelukast) | No glycemic effect |
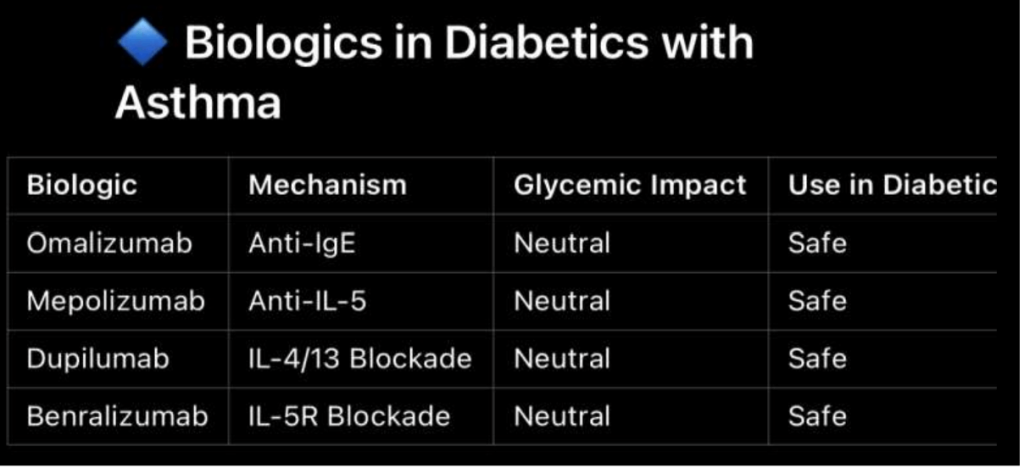
| Refractory | Biologics (omalizumab, mepolizumab, dupilumab) | No impact on blood sugar → ideal in diabetics |
| Rescue | Use short-acting beta agonists (SABA) like salbutamol | Use with caution – may cause hyperglycemia via β2-agonist effect |
Breathless and Sweet – Recent Advances
1. Metformin
- Evidence: A large UK JAMA Internal Medicine study (2024–25) reported that metformin use was linked with a 24–32% reduction in asthma exacerbations in T2DM patients, independent of BMI or HbA1c.
- Mechanism: Activates AMPK, suppresses airway inflammation by reducing IL-6, TNF-α, NF-κB activity.
2. GLP-1 Receptor Agonists (GLP-1RAs) – liraglutide, semaglutide
- Evidence: When added to metformin, GLP-1RAs achieved an additional ~40% reduction in asthma attacks (Incidence Rate Ratio ~0.60).
- Mechanism: Lower airway inflammation, enhance lung function, particularly beneficial in obese and diabetic asthma phenotypes.
Emerging Therapies – Asthma in Diabetes
3. SGLT-2 Inhibitors
- Evidence: Meta-analyses suggest slightly fewer asthma-related serious adverse events compared to placebo.
- Mechanism: May reduce systemic inflammation (↓ TNF-α, IL-6).
- Real-world data: Asthma exacerbation rates were comparable or slightly lower than with metformin.
4. Tezepelumab (Anti-TSLP Biologic)
- Regulatory status: Approved in US (2021) and EU (2022) for severe, uncontrolled asthma.
- Effect: Reduces exacerbations across all phenotypes (both T2 and non-T2 asthma).
- Relevance in diabetics: Provides a non-steroid targeted therapy, minimizing glycemic concerns.
5. Dexpramipexole (Oral Eosinophil-Lowering Agent)
- Investigational: Shown to reduce eosinophil counts and act as a steroid-sparing therapy.
- Potential role: Promising for eosinophilic asthma, especially in diabetic patients where avoiding systemic steroids is crucial
Beyond Inhalers – Asthma in Diabetes
- Macrolide Therapy (e.g., Azithromycin):
- Recommended by GINA for severe, refractory asthma, especially non-eosinophilic phenotypes.
- Provides anti-inflammatory benefit, helps reduce steroid exposure, thereby indirectly protecting glycemic control.
- Metformin & GLP-1 Receptor Agonists:
- Show promising anti-asthma effects independent of their glycemic benefits.
- Improve airway inflammation and reduce exacerbations.
- Advanced Biologics & Emerging Agents:
- Tezepelumab (anti-TSLP): Effective across T2 and non-T2 asthma phenotypes.
- Dexpramipexole (investigational): Oral eosinophil-lowering, steroid-sparing—valuable for diabetic patients.
- Lifestyle Interventions:
- Weight management, diet, exercise act synergistically with pharmacotherapy.
- Address both asthma control and metabolic health.
Case Summary
- Patient: 58-year-old male, poorly controlled Type 2 Diabetes (HbA1c 9.2%)
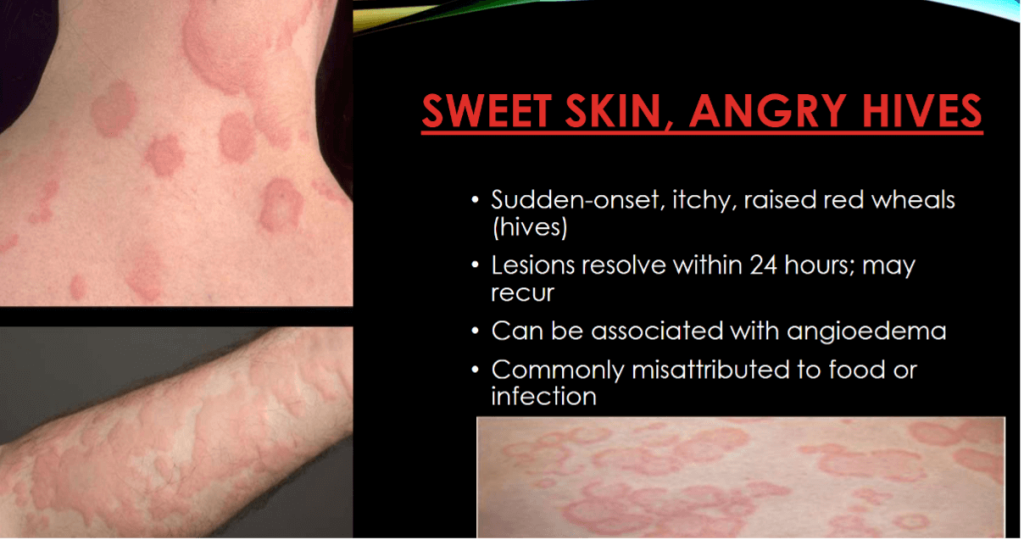
- Presentation: Daily urticaria for 3 weeks
- Meds: Metformin, Insulin glargine (long-standing, no new meds)
- Workup:
- Skin biopsy → perivascular eosinophils + dermal edema (consistent with urticaria)
- Normal tryptase (rules out systemic mastocytosis)
- Negative ANA (no connective tissue overlap)
Option Analysis
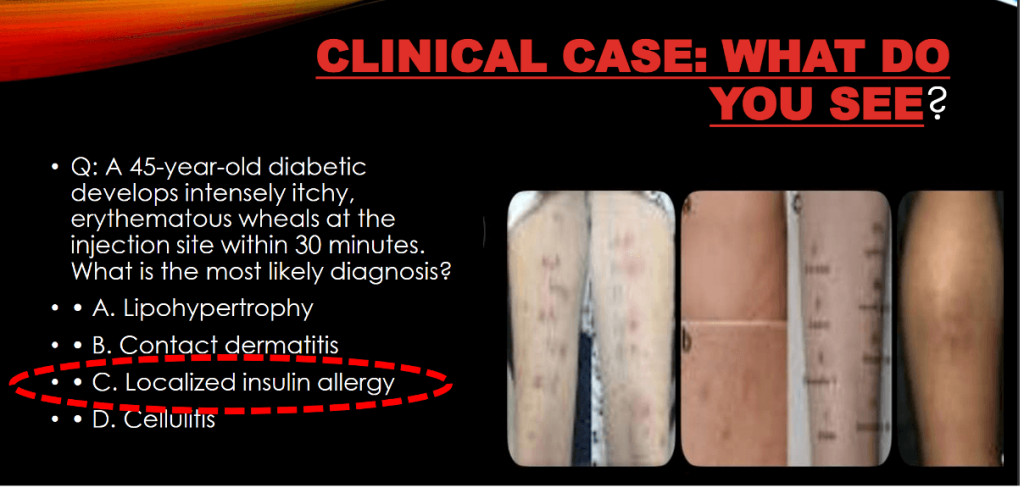
A) IgE-mediated histamine release triggered by insulin analogs
- Insulin allergy is possible but usually presents early after insulin initiation (local erythema, angioedema, systemic reaction).
- This patient is long on insulin, no new agent, so less likely.
B) Immune complex deposition secondary to glycation end-products
- AGE (advanced glycation end-products) play a role in vascular damage, but immune complex vasculitis is not the mechanism of chronic urticaria.
- Not supported by biopsy findings.
C) Mast cell destabilization due to advanced glycation end-products and metabolic inflammation
- Most plausible in diabetes-related chronic urticaria.
- Poor glycemic control → AGEs + systemic inflammation (IL-6, TNF-α) → mast cell activation/destabilization → histamine release.
- Fits biopsy (mast cell/eosinophil mediated) and chronic course.
D) Delayed-type hypersensitivity reaction to metformin metabolites
- Metformin rarely causes cutaneous reactions, usually exanthematous/maculopapular rash, not recurrent urticaria.
- Very uncommon, so less likely.
Correct Answer: C) Mast cell destabilization due to advanced glycation end-products and metabolic inflammation
Clinical Pearl: Chronic urticaria is more common in diabetics, especially with poor glycemic control, due to immune dysregulation, systemic inflammation, and mast cell priming by AGEs. Optimizing glycemic control is often part of symptom management.
Antidiabetic Drugs That May Trigger Urticaria
- SGLT2 Inhibitors – Canagliflozin, Dapagliflozin
- DPP-4 Inhibitors – Sitagliptin, Linagliptin
- Sulfonylureas – Glimepiride
- Thiazolidinediones – Pioglitazone
- Insulin Analogs – particularly long-acting formulations (e.g., glargine, detemir)
Safe Treatment Options (Without Affecting Glucose Levels)
- Discontinue suspected antidiabetic drug → switch to a safe alternative
- Non-sedating antihistamines (Cetirizine, Loratadine) → first-line & safe
- Short-course corticosteroids → use only if necessary, monitor closely (may raise glucose)
- Omalizumab → effective in chronic urticaria, no glycemic impact
- Montelukast → useful adjunct, safe in diabetes
Algorithm: Urticaria Management in Diabetes
- Identify new-onset rash → take detailed history & examination
- Review medications → suspect antidiabetic drug?
- Common culprits: SGLT2 inhibitors, DPP-4 inhibitors
- If yes → discontinue suspected agent
- Start treatment
- Non-sedating antihistamines (first-line)
- ± Short course corticosteroids (if severe, monitor glucose)
- Switch to safe alternative antidiabetic drug → ensure glycemic stability
- If persistent/refractory →
- Consider Omalizumab
- Refer to allergy specialist
- Further workup → skin/blood-based diagnostics (IgE, eosinophils, tryptase, biopsy if needed)
What is the most probable immunologic mechanism responsible for the reaction?
Options:
A) Type II – Antibody-mediated cytotoxic
B) Type I – IgE-mediated hypersensitivity
C) Type III – Immune complex–mediated
D) Type IV – T-cell–mediated hypersensitivity
Correct Answer: B) Type I (IgE-mediated hypersensitivity)
Explanation
- Chronic urticaria / drug-induced urticaria is typically driven by mast cell degranulation and histamine release, often through an IgE-mediated pathway.
- Type II (cytotoxic) → more relevant to hemolysis, thrombocytopenia, etc.
- Type III (immune complex) → seen in vasculitis, serum sickness, not urticaria.
- Type IV (delayed T-cell–mediated) → eczematous or contact dermatitis-type reactions, not classic urticaria.
Clinical Pearl: In diabetics, metabolic inflammation + advanced glycation end products (AGEs) may further destabilize mast cells, amplifying this Type I response.
When The Cure Bites Back – Insulin Allergy
Incidence & Background
- Occurs in ~5–7% of insulin users
- Frequently due to excipients such as protamine or metacresol
- Modern highly purified insulin analogs have reduced risk, but reactions still occur
- Clinical presentation may be:
- Local (erythema, induration at injection site)
- Systemic (urticaria, angioedema, anaphylaxis – rare)
Clinical Presentation – Insulin Allergy
- Immediate (Type I, IgE-mediated):
- Localized wheals, itching, swelling at injection site
- Delayed (Type III/IV):
- Nodules, granulomas, induration at injection site
- Severe/Systemic reactions:
- Generalized urticaria, angioedema, or anaphylaxis (rare but life-threatening)
Diagnostic Tools – Insulin Allergy
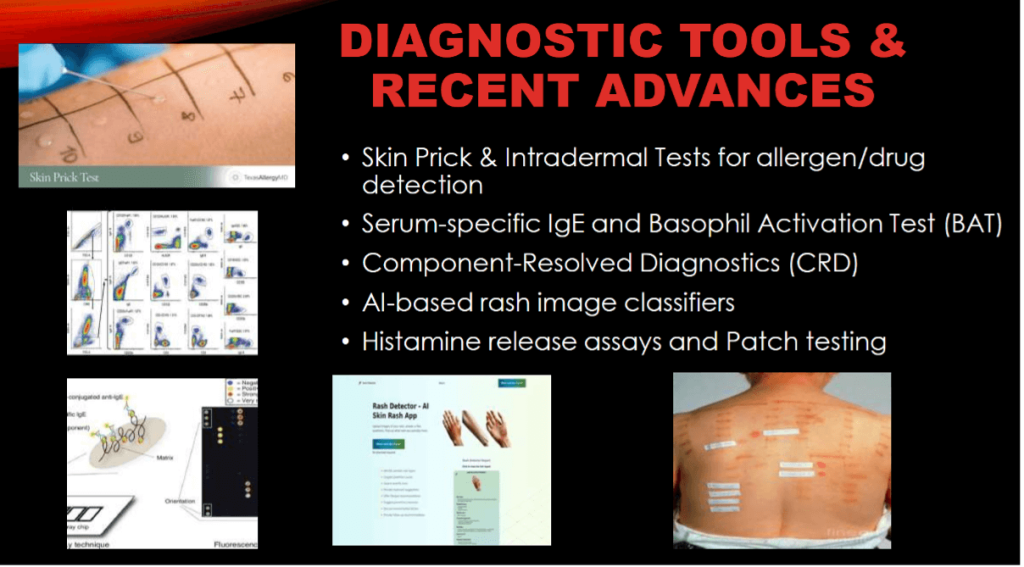
- Skin Prick & Intradermal Testing → to detect immediate IgE-mediated reactions
- Serum Insulin-Specific IgE → supportive evidence for Type I hypersensitivity
- Patch Testing (for excipients) → identifies allergy to additives such as protamine, zinc, metacresol
- Drug Provocation Test (controlled setting) → gold standard when diagnosis remains uncertain, performed under strict medical supervision
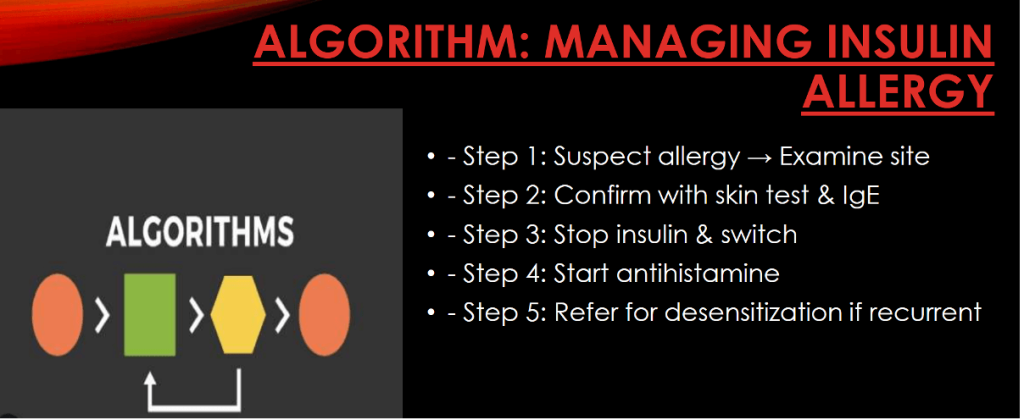
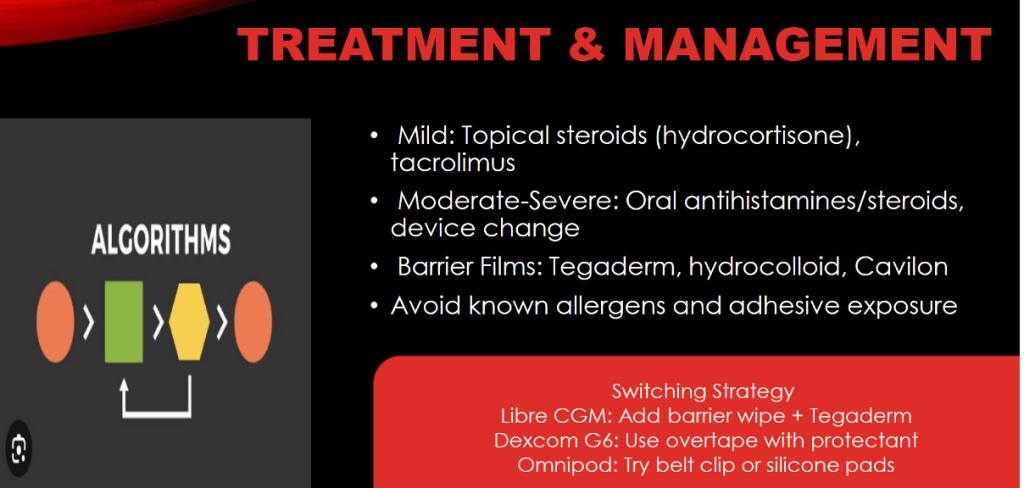
Treatment & Management – Insulin Allergy
- Discontinue the suspected insulin preparation
- Switch to a different formulation → e.g., human insulin analogs or preparations without the offending excipient
- Symptomatic relief:
- Non-sedating antihistamines (first-line)
- Short corticosteroid course if severe (use cautiously in diabetes)
- Desensitization protocols – for patients requiring insulin with no safe alternative
- Consider excipient-free formulations (e.g., avoid protamine/metacresol) where available
Recent Advances – Insulin Allergy Management
- Continuous Glucose Monitoring (CGM):
Enables safe transition to non-insulin regimens and close tracking of glycemic fluctuations during allergy workup. - Monoclonal Antibody Therapy (e.g., Omalizumab):
Effective in severe IgE-mediated insulin allergy, reduces reliance on systemic steroids. - Recombinant Human Insulin (without Protamine):
Minimizes risk of excipient-induced hypersensitivity. - Skin Patch Bio-identifiers:
Emerging technology for drug tracing and allergy monitoring, helping identify culprit molecules.
Case Summary
- Patient: 15-year-old boy with Type 1 Diabetes Mellitus
- Device: FreeStyle Libre CGM, 6 months
- Issue: Pruritic, erythematous, eczematous rash at adhesive site after 3rd sensor use
- Patch test: Positive for isobornyl acrylate (a known allergen in some CGM adhesives)
- Impact: Poor glycemic control due to reluctance to use CGM
Options
A. Discontinue sensor use permanently and switch to fingerstick monitoring
- Not ideal → CGM offers superior glucose monitoring and quality of life. Permanent discontinuation is not first-line.
B. Start systemic steroids and continue the same sensor brand
- Inappropriate for long-term management in a child. Systemic steroids carry significant risks, especially in diabetes.
C. Apply barrier film, switch to a different CGM device, and consider topical tacrolimus
- Best option: Barrier films or hydrocolloid dressings can reduce direct allergen exposure.
- Switching to a different CGM brand (without isobornyl acrylate) is recommended.
- Topical tacrolimus (or corticosteroids in short courses) may help manage dermatitis safely.
D. Rotate sensor sites and monitor for further reactions
- Site rotation alone will not prevent recurrence, since allergen exposure persists.
Correct Answer: C. Apply barrier film, switch to a different CGM device, and consider topical tacrolimus
Clinical Pearl
- Isobornyl acrylate allergy is increasingly recognized with adhesive devices (CGM, insulin pumps).
- Management:
- Barrier protection
- Switching to alternative devices (e.g., Dexcom G6/G7, Eversense)
- Topical non-steroidal immunomodulators for skin care
Sticking to Trouble: Allergic Reactions to Insulin Delivery Adhesives
Why This Matters
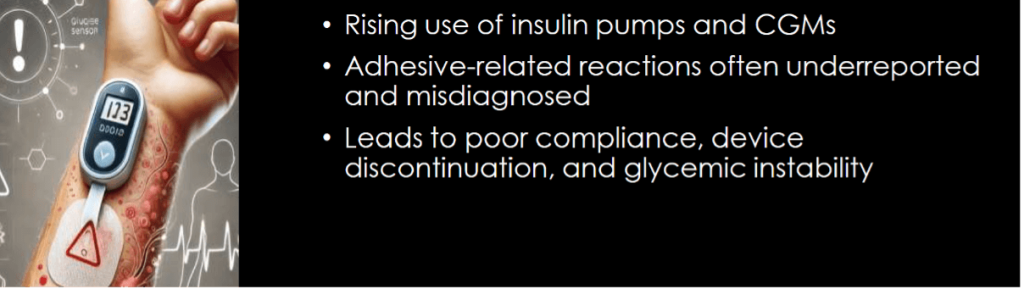
Prevalence – Device-Related Allergies in Diabetes
- Insulin devices (pens, pumps): Contact dermatitis in ~10–35% of users
- CGM systems (Libre, Dexcom, Medtronic): Up to 50% report local skin irritation
- High-risk groups:
- Type 1 diabetics (long-term device dependence)
- Children/adolescents (sensitive skin)
- Atopic individuals (eczema, allergic rhinitis, asthma)
Types of Skin Reactions with Diabetes Devices
- Irritant Contact Dermatitis
- Non-immune reaction
- Redness, dryness, itching at adhesive site
- Allergic Contact Dermatitis
- Delayed Type IV hypersensitivity
- Often due to acrylates/excipients in adhesives
- Urticarial Reaction
- Immediate (Type I, IgE-mediated)
- Wheals, swelling, itching; rarely systemic
- Granulomatous / Eczematous Reactions
- Result of chronic exposure
- Persistent eczema-like or nodule-forming lesions
Pathophysiology – Device-Related Skin Reactions
Allergic Contact Dermatitis (Type IV Hypersensitivity)
- Triggered by sensitization to adhesive/excipient components such as:
- Acrylates (e.g., isobornyl acrylate in CGM sensors)
- Colophony (rosin derivatives)
- Rubber compounds
- Mediated by T-cell immune response → delayed inflammation and eczematous rash
Irritant Contact Reactions (Non-Immune)
- Caused by mechanical or chemical irritation rather than immune sensitization
- Mechanisms:
- Occlusion of skin under adhesive
- Sweat accumulation and maceration
- Direct chemical irritation from adhesives or disinfectants
Diagnosis in OPD Setup – Device-Related Dermatitis
- History:
- Temporal relation of rash with device/patch use
- Symptom pattern (onset, recurrence, worsening with reapplication)
- Physical Examination:
- Rash localized to adhesive/contact site
- Look for erythema, papules, vesicles, or chronic lichenified eczema
- Patch Testing:
- Test for common allergens: acrylates (e.g., isobornyl acrylate), colophony, rubber compounds
- Documentation:
- Clinical photographs for baseline and follow-up comparison
- Useful for monitoring progression and medicolegal clarity
Newer Advances – Device-Related Allergy Management
- Acrylate-free adhesives → e.g., Dexcom G7, reducing risk of contact dermatitis
- Anti-allergic polymer tapes → alternative hypoallergenic dressings for CGM/insulin devices
- AI-based patch compatibility analysis → predictive tools to match patient skin profile with safe adhesives
- Experimental microneedle insulin delivery systems → bypass adhesives, reduce risk of dermatitis
Special Considerations (Pediatric / Atopic Patients)
- Higher risk of adhesive-related skin reactions
- Use lowest potency topical steroids if needed
- Avoid systemic steroids in children
- Preventive strategies: Cavilon™ or barrier sprays before device application
Further Reading:
- Oh J, Vasquez EC, Alvarez-Arango S, Ramesh M, Castells MC. Insulin Allergy: The Allergist’s Updated Approach to Evaluation and Management. J Allergy Clin Immunol Pract. 2025 May;13(5):990-999. doi: 10.1016/j.jaip.2025.02.028. Epub 2025 Mar 1. PMID: 40032231.
- Lu G, Wang Y, Huang H, et al. Association Between Diabetes Mellitus and Allergic Diseases Sensitized by Different Allergens and the Potential Mechanism of Diabetes Mellitus Affecting Ovalbumin-Induced Allergic Rhinitis. American Journal of Rhinology & Allergy. 2025;39(4):271-283. doi:10.1177/19458924251332786
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
I apologize for including a link, but I believe it will help clarify my question. Given the information in the article about the use of Fluticasone nasal spray for managing allergic rhinitis in diabetic patients, could you elaborate on its mechanism of action and any potential side effects? For more details, you can refer to this link: https://pillintrip.com/medicine/fluticasone-nasal. Thank you!