
CME INDIA Case Presentation by Dr. Sikandar Singh, Consultant Physician, Deoghar.
CME INDIA Case Study
Quick Look
Systolic Anterior Motion of Posterior Mitral Leaflet in Hypertrophic Cardiomyopathy with Mild Subaortic Obstruction: Rare Case Note
How Presented?
A middle-aged female patient presented with progressive tiredness and exertional shortness of breath of approximately one year duration. There was no history of syncope, chest pain, or palpitations. Obstetric history was uneventful. No prior known structural heart disease had been documented.
Blood pressure at evaluation was 130/70 mmHg. Routine biochemical investigations including renal function were within normal limits.
What Electrocardiography demonstrated
Left ventricular strain pattern.
Echocardiographic Findings
Images and videos:

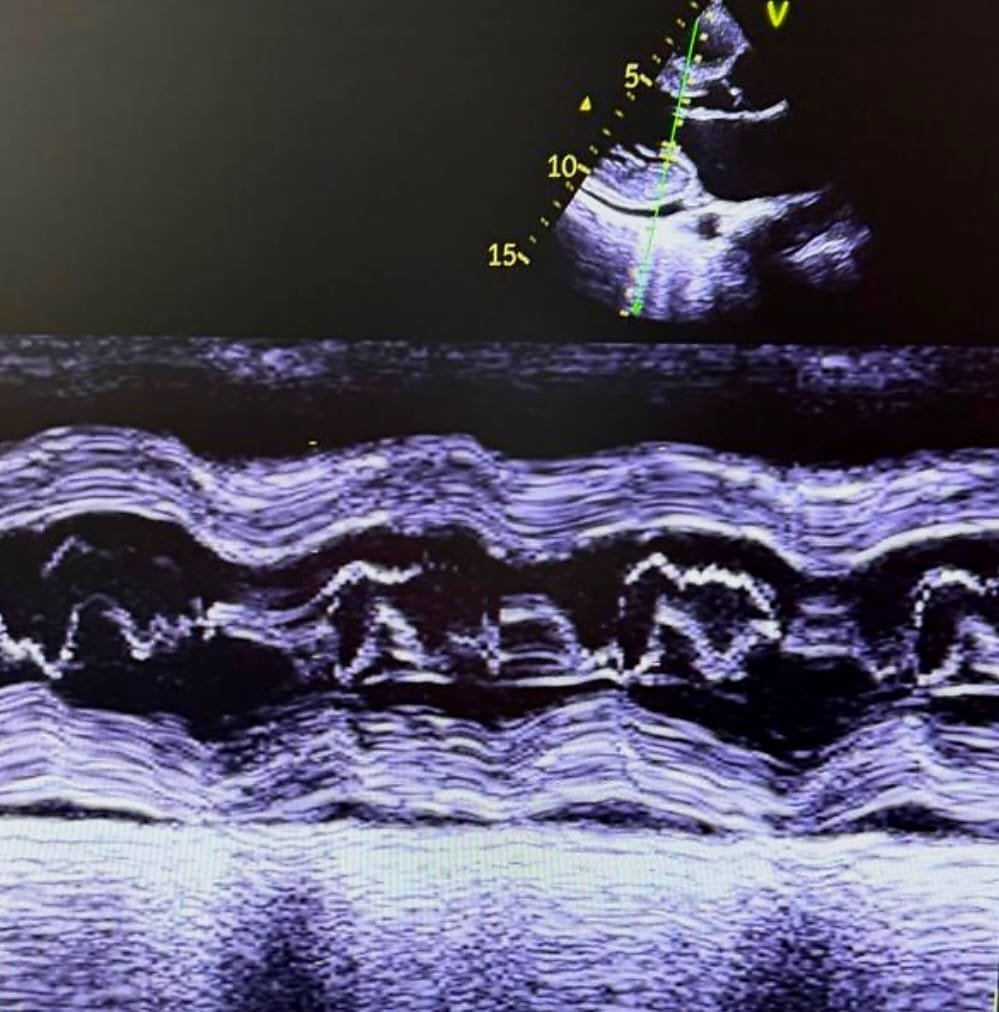
| Echocardiography revealed: |
| Features consistent with hypertrophic cardiomyopathy |
| Systolic anterior motion (SAM) of the posterior mitral leaflet (PML) |
| Dynamic LVOT obstruction |
| LVOT mean pressure gradient: |
| 14 mmHg at rest |
| 20 mmHg on Valsalva |
| Mild subaortic obstruction |
| Mild pulmonary arterial hypertension |
| Right ventricular diastolic dysfunction |
| Mild pericardial effusion |
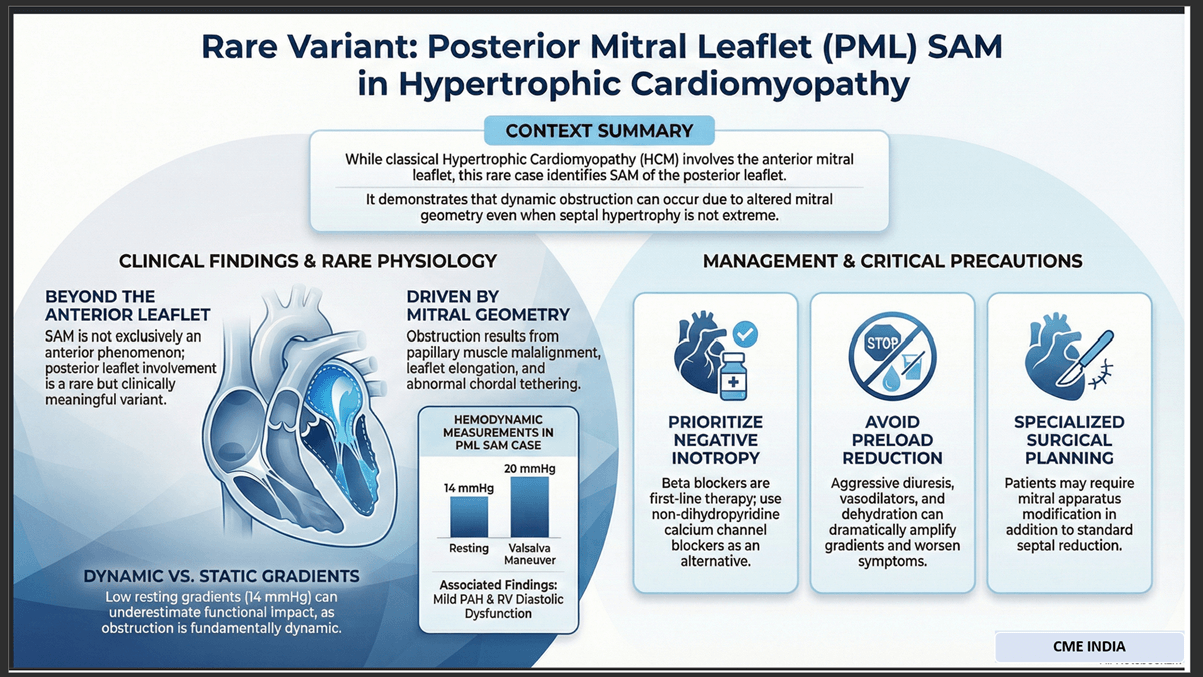
Notably, SAM involved the posterior mitral leaflet — an uncommon variant — rather than the classical anterior leaflet SAM seen in obstructive HCM.
Let us Analyse echocardiographic finding
This case is unusual for several reasons.
- Classic hypertrophic cardiomyopathy–related obstruction is mediated by SAM of the anterior mitral leaflet, where Venturi forces and drag pull the leaflet into the septum during systole. Posterior leaflet involvement indicates altered mitral apparatus geometry, suggesting:
- Papillary muscle malalignment
- Abnormal chordal tethering
- Leaflet elongation
- Septal–mitral interaction distortion
- Posterior leaflet SAM is rare and often under-recognized. It may produce dynamic LVOT obstruction even when septal hypertrophy is not extreme. The modest gradient in this patient suggests early or compensated obstruction, which may become hemodynamically significant under stress, dehydration, tachycardia, or reduced preload.
- The coexistence of mild PAH, RV diastolic dysfunction, chronic exertional dyspnea, indicates evolving hemodynamic consequences.
Importantly, symptoms correlate more with dynamic physiology than static gradient numbers.
Clinical Significance
| This case highlights that: |
| SAM is not exclusively an anterior leaflet phenomenon |
| Posterior leaflet SAM can produce clinically meaningful obstruction |
| LVOT gradient alone underestimates functional impact |
| Early recognition prevents progression and inappropriate management |
These patients may worsen with:
- Diuretics
- Vasodilators
- Dehydration
- Tachyarrhythmias
Management must prioritize negative inotropy and preload preservation.
| Management Considerations |
| Beta blockers as first-line therapy |
| Non-dihydropyridine calcium channel blockers if needed |
| Avoid aggressive diuresis |
| Avoid vasodilators that reduce preload |
| Serial echocardiographic follow-up |
| Referral to HCM center if gradient progresses |
Surgical decision-making differs in posterior leaflet SAM cases because mitral apparatus modification may be required in addition to septal reduction.
Comments by Dr. Deepak Gupta, DM (Cardiology), Samford Hospital, Ranchi:
The four-chamber echocardiographic view demonstrates biventricular involvement along with associated pericardial effusion. In this clinical context, cardiac MRI represents a crucial diagnostic investigation, providing comprehensive structural and tissue characterization.
Approximately 10% of patients with hypertrophic obstructive cardiomyopathy (HOCM) exhibit systolic anterior motion (SAM) of the posterior mitral leaflet (PML) as a significant contributor to severe subaortic obstruction. In some cases, PML-SAM may coexist with the more commonly observed anterior mitral leaflet (AML) SAM.
PML-SAM typically results from structural abnormalities of the posterior mitral leaflet, particularly elongation of the middle scallop. Surgical management, when indicated, includes posterior leaflet plication with edge-to-edge repair to relieve left ventricular outflow tract obstruction and restore mitral valve competence.
CME INDIA Learning Edge
- This case illustrates a rarely appreciated variant of obstructive physiology in hypertrophic cardiomyopathy (HCM) — systolic anterior motion (SAM) involving the posterior mitral leaflet (PML). Classical teaching frames LVOT obstruction as a consequence of anterior leaflet–septal interaction, yet contemporary echocardiographic literature confirms that altered mitral apparatus geometry alone can generate dynamic obstruction even when septal hypertrophy is modest. Posterior leaflet SAM likely reflects a complex interplay of papillary muscle displacement, elongated leaflets, and abnormal chordal tension, producing systolic drag forces sufficient to narrow the outflow tract.
- The relatively low resting gradient in this patient should not be interpreted as benign. HCM obstruction is fundamentally dynamic, and symptom burden often correlates more with loading conditions than with static Doppler measurements. Dehydration, tachycardia, or pharmacologic preload reduction can dramatically amplify gradients. The presence of mild pulmonary hypertension and right ventricular diastolic dysfunction suggests chronic hemodynamic stress and supports the clinical relevance of the obstruction despite numerically modest gradients.
- Recognition of posterior leaflet SAM has practical consequences. Standard heart failure approaches — particularly diuretics and vasodilators — may worsen obstruction by reducing preload. Management should instead emphasize negative inotropy and ventricular filling optimization, with beta blockers as first-line therapy. Importantly, surgical planning in such variants may require mitral apparatus intervention in addition to septal reduction, underscoring the need for expert echocardiographic assessment and referral to specialized HCM centers when symptoms progress.
- This case reinforces a critical principle: in HCM, anatomy explains physiology, but physiology explains symptoms.
CME INDIA Quick Learning Points
✅ Not all SAM is anterior leaflet SAM
✅ Posterior leaflet SAM is rare but real
✅ Symptoms may precede large LVOT gradients
✅ Dynamic physiology matters more than numbers
✅ Mitral geometry drives obstruction
✅ Avoid preload-reducing drugs
✅ Beta blockers are protective
✅ Echo expertise is diagnostic
✅ Early recognition changes management
References:
- Ommen SR, Mital S, Burke MA, et al. 2024 AHA/ACC guideline for the diagnosis and treatment of hypertrophic cardiomyopathy. Circulation. 2024;149:e1–e82.
- Sherrid MV, Wang J, Kim B, et al. Mitral valve mechanisms of left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2023;82:1235–1248.
- Geske JB, Ommen SR, Gersh BJ. Hypertrophic cardiomyopathy: clinical update 2025. Lancet. 2025;405:412–424.
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs