
CME INDIA Presentation by Dr. Arvind Gupta, MBBS, MD, FRCP (Glasgow), FRCP (Edin), FICP, FACE, FRSSDI, F Diab India. Senior Consultant and Head – Department of Internal Medicine and Diabetes, RHL-Rajasthan Hospital, Jaipur.
Based on presentation at CID 02 on 17/08/2024, Mumbai, Bharat.
Diabetes: A Global EmergencyWhat is Sarcopenic obesity?
- 537 million adults aged 20-79 years (1 in 10) are currently living with diabetes. This figure is expected to increase to 643 million by 2030 and **784 million by 2045.
- Diabetes caused 6.7 milliondeaths in 2021, equivalent to one death every five seconds.
- Prediabetes, a hidden epidemic, affects 541 million adults, representing 10.6% of the population with Impaired Fasting Glucose, and 319 million adults, or 6.2%, with Impaired Glucose Tolerance.
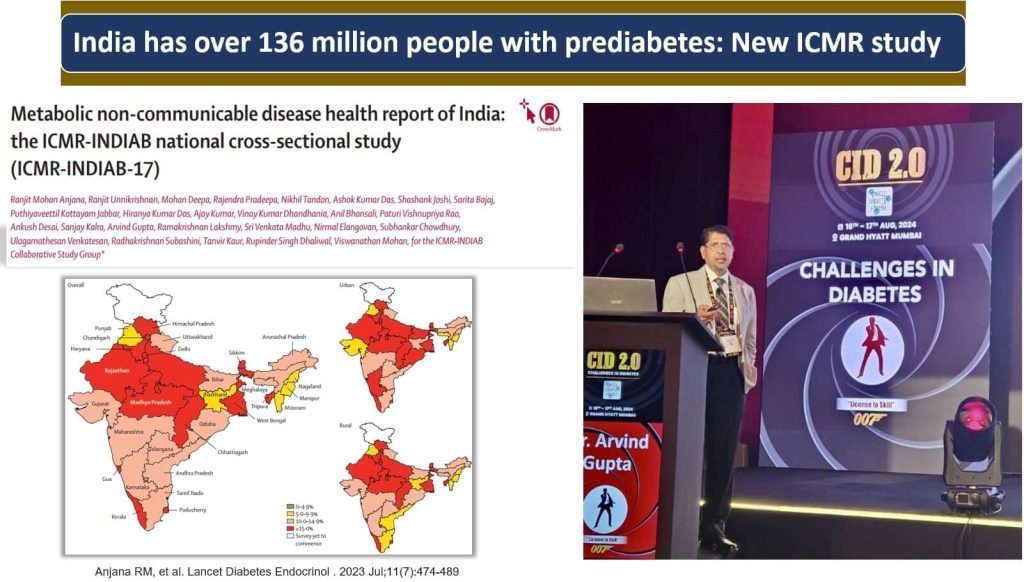
In India, the prevalence of prediabetes
- Highest in the central and northern regions.
- Lowest in Punjab, Jharkhand, and parts of the northeastern region.
- There was no significant difference in the prevalence of prediabetes between urban and rural areas.
Prediagnosis of Type 2 Diabetes Mellitus
- Prediabetes is not a disease.
- It is a prediagnosis of diabetes.
- A warning sign.
- “Prediabetes should not be viewed as a clinical entity in its own right but rather as an increased risk for diabetes and cardiovascular disease (CVD)”* — American Diabetes Association.
Approximately 50% β-cell function is lost at diagnosis of prediabetes
- Can Diabetes be Reversed?
- What exactly is Diabetes Reversal?
- Is it Reversal or Remission?
Reversal or Remission?
- Remission implies achieving normal HbA1c levels without the need for any anti-diabetic medications.
- Reversal could also mean a reduction in the number or dosage of anti-diabetic medications. For instance, transitioning from an insulin-requiring stage to a non-insulin-requiring stage of the condition. Reversal of diabetes typically results from an improvement in insulin sensitivity.
The American Diabetes Association (ADA) defines the following three mutually exclusive states of remission:
Partial remission = Subdiabetic hyperglycemia of at least 1 year
- A1C level not diagnostic of diabetes [5.7–6.4%; 39–46 mmol/mol].
- Fasting glucose level 100–125 mg/dL [5.6–6.9 mmol/L]).
Complete remission = Normoglycemia of at least 1 year
- A1C level in the normal range [<5.7%; <39 mmol/mol]
- Fasting glucose <100 mg/dL [5.6 mmol/L])
Prolonged remission (or “cure”) = Complete remission of at least 5 years
Management for Prediabetes
- Non-Pharmacological.
- Pharmacological.
Non-pharmacological Management
People with prediabetes should modify their lifestyle including:
- Attempts to lose 5 to 10% of body weight if overweight or obese.
- Participate in moderate physical activity (e.g., walking) for at least 150 mins/week.
- 6–8 h of sleep daily.
- Healthy lifestyle measures including diet and physical activity are equally important for non-obese patients with pre-diabetes.
- Clinical trials/outcome studies of MNT have reported decreases in HbA1c (A1C) of ≈1% in type 1 diabetes and 1–2% in type 2 diabetes, depending on the duration of diabetes.
Clinical Pearls on the Twin Cycle Hypothesis for Diabetes Remission
- The Twin Cycle Hypothesis posits that Type 2 diabetes results from a vicious cycle between the liver and pancreas. Excess fat accumulation in the liver leads to increased hepatic glucose production, causing elevated insulin levels. This, in turn, prompts the pancreas to store more fat, impairing its function.
- A low-calorie diet can interrupt the twin cycles by has been shown to induce remission in some patients with Type 2 diabetes.
- The hypothesis suggests that diabetes remission is more likely if the twin cycles are disrupted early in the disease process. Thus, early and aggressive lifestyle interventions may significantly increase the chances of diabetes reversal.
- The primary mechanism through which remission is achieved under the Twin Cycle Hypothesis is substantial weight loss, leading to a reduction in visceral and liver fat. This highlights the importance of sustained weight management in managing and potentially reversing Type 2 diabetes.
- Not all patients respond to dietary interventions the same way, indicating the need for personalized treatment plans. Regular monitoring of liver fat, pancreatic function, and overall metabolic health is essential for optimizing remission strategies.
- Maintaining remission requires continuous lifestyle management to prevent the re-accumulation of fat in the liver and pancreas. Ongoing support and monitoring are crucial to ensure that the improvements are sustained over the long term.
- Type 2 diabetes is a reversible condition of intra-organ fat excess to which some people are more susceptible than others.
The DiRECT (Diabetes Remission Clinical Trial) demonstrated that Type 2 diabetes remission is achievable through intensive weight management.
- The study focused on a low-calorie, nutrient-balanced diet, leading to significant weight loss.
- A large proportion of participants achieved and maintained remission of diabetes for up to two years, emphasizing the effectiveness of weight loss in diabetes management.Weight loss led to a reduction in liver and pancreatic fat, improving insulin sensitivity and function, which is crucial for maintaining glucose control. The success rate was higher in participants who had been diagnosed with diabetes for a shorter period, indicating the benefits of early and aggressive intervention.
- These findings underscore the potential for diabetes remission through structured weight loss programs, shifting the treatment paradigm for Type 2 diabetes from management to possible remission.
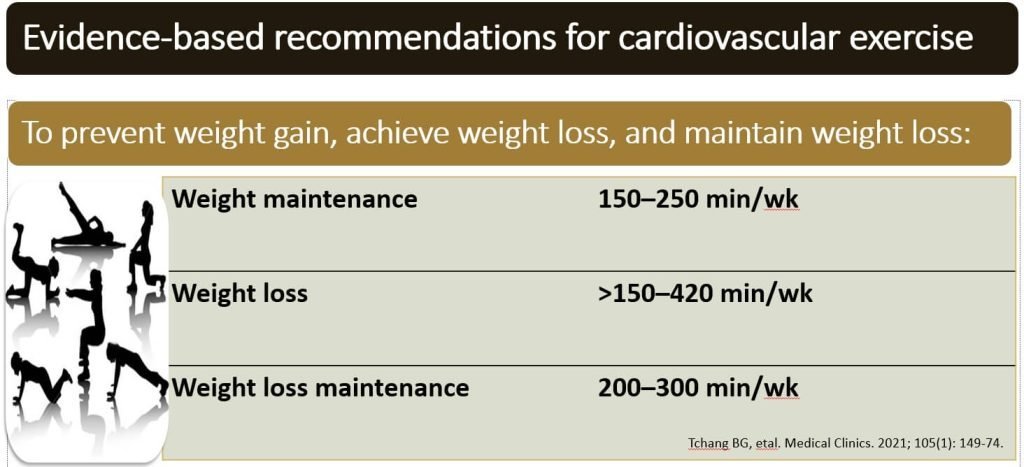
Lifestyle Modifications: Physical Activity
- Role of physical activity in weight management is 2-fold: to support an energy deficit and to preserve lean muscle mass.
- Total energy expenditure (TEE) is partitioned into basal metabolic rate (BMR), diet-induced thermogenesis (DIT), nonexercise activity thermogenesis (NEAT), and exercise.
- Exercise, both cardiovascular and resistance training (RT), is the only component of TEE that is significantly modifiable.
- The combination of diet and exercise always results in greater weight loss than either modality alone.
Role of Yoga in Prediabetes
- Practice of yoga is a promising adjuvant along with exercise.
- Diabetes-related physiological effects of yoga are reduction in:
- Fasting and postprandial blood glucose.
- Total cholesterol, low-density lipoprotein (LDL) [bad cholesterol].
- Blood pressure and heart rate.
- Reduction in body weight (waist/hip ratio).
- Practise of meditation when done along with exercise relieves stress, depression and anxiety.
- Improvement in patient’s attitude and self-control.
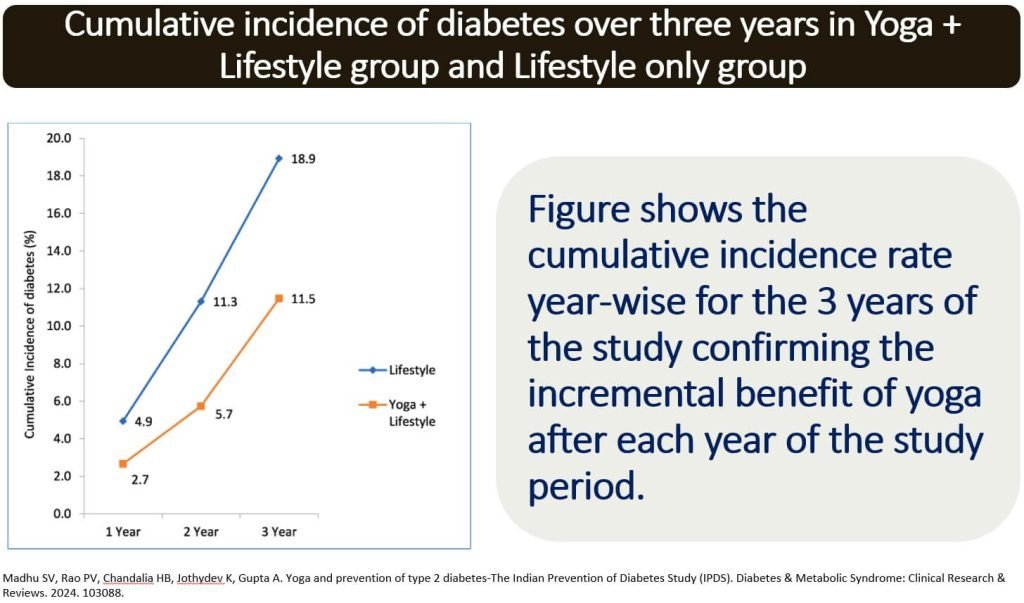
- This randomized controlled trial evaluated the long-term effectiveness of yoga in reducing the risk of Type 2 diabetes among adults with prediabetes. Over a 3-year period, 974 participants were assigned to either a group receiving a structured yoga intervention plus standard lifestyle measures (group 1) or a group receiving lifestyle measures alone (group 2).
- The group that practiced yoga had a 39.2% lower relative risk of developing Type 2 diabetes compared to the lifestyle-only group (11.5% incidence in group 1 vs. 18.9% in group 2).
- The odds of developing diabetes were 1.74 times higher in the lifestyle-only group compared to the yoga group.
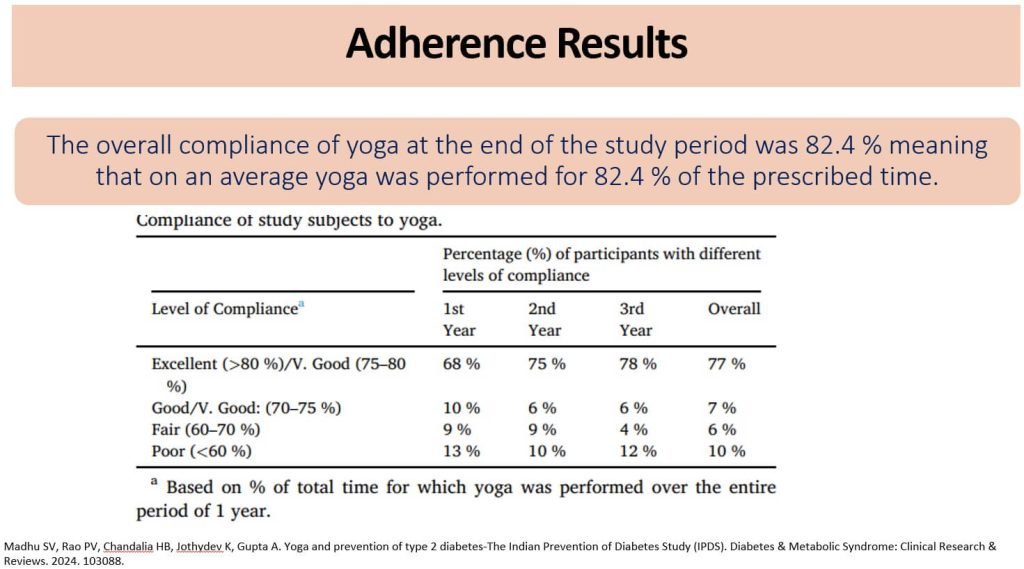
- Compliance with the yoga regimen was high, with 77% of participants performing yoga regularly.
- Incorporating structured yoga into standard lifestyle measures significantly reduces the risk of Type 2 diabetes in individuals with prediabetes, making it a beneficial addition to lifestyle interventions.
- This study assessed the impact of a 24-week yoga intervention on various health markers in patients with Type 2 diabetes. It involved 104 participants who were randomly divided into two groups: a control group and an intervention group, which performed 40 minutes of yoga exercises five days a week.
- After 24 weeks, the intervention group had a lower body mass index (BMI), reduced waist-hip ratio, and decreased systolic blood pressure compared to the control group.
- Participants in the yoga group showed significantly lower fasting glucose levels and glycated hemoglobin (HbA1c), indicating improved blood sugar control.
- The yoga group had reduced levels of low-density lipoprotein (LDL) cholesterol and non-high-density lipoprotein (non-HDL) cholesterol, along with higher levels of high-density lipoprotein (HDL) cholesterol.
- Inflammatory markers such as interleukin-6 (IL-6) and high-sensitivity C-reactive protein (hs-CRP) were significantly lower in the yoga group.
- The intervention group had higher levels of serum total antioxidants.
- Conclusion:A 24-week yoga intervention resulted in significant improvements in glycemic control, lipid profile, inflammation, and antioxidant levels in patients with Type 2 diabetes, suggesting that yoga can be an effective complementary therapy for managing this condition.
Follow-up Counseling
- Shown to be important to success.
- Monitor weight loss progress.
- Provide ongoing counseling for lifestyle modification,
- Consider pharmacologic therapy (e.g., metformin) if appropriate.
- Provide annual screenings for the development of diabetes:
- Every 12 months for those with prediabetes.
- Every 3 years if screening is negative.
- Continually screen for modifiable risk factors at each interaction.
CME INDIA Tips for taking control
| Lose extra weight |
| Be more physically active |
| Eat healthy fibrous foods |
| Eat healthy fats |
| Skip fad diets and make healthier choices |
CME INDIA Tail-Piece
References:
- https://diabetesatlas.org/atlas/tenth-edition/
- Anjana RM, Unnikrishnan R, Deepa M, Pradeepa R, Tandon N, Das AK, Joshi S, Bajaj S, Jabbar PK, Das HK, Kumar A, Dhandhania VK, Bhansali A, Rao PV, Desai A, Kalra S, Gupta A, Lakshmy R, Madhu SV, Elangovan N, Chowdhury S, Venkatesan U, Subashini R, Kaur T, Dhaliwal RS, Mohan V; ICMR-INDIAB Collaborative Study Group. Metabolic non-communicable disease health report of India: the ICMR-INDIAB national cross-sectional study (ICMR-INDIAB-17). Lancet Diabetes Endocrinol. 2023 Jul;11(7):474-489. doi: 10.1016/S2213-8587(23)00119-5. Epub 2023 Jun 7. PMID: 37301218.
- Rett, Kristian, and Ulrike Gottwald-Hostalek. “Understanding prediabetes: definition, prevalence, burden and treatment options for an emerging disease.” Current medical research and opinion 35.9 (2019): 1529-1534.
- Buse JB, Caprio S, Cefalu WT, Ceriello A, Del Prato S, Inzucchi SE, McLaughlin S, Phillips GL 2nd, Robertson RP, Rubino F, Kahn R, Kirkman MS. How do we define cure of diabetes? Diabetes Care. 2009 Nov;32(11):2133-5. doi: 10.2337/dc09-9036. PMID: 19875608; PMCID: PMC2768219.
- https://rssdi.in/new/pdf/Vol-38-Supplement-1_March2018.pdf
- Taylor R. Banting Memorial lecture 2012: reversing the twin cycles of type 2 diabetes. Diabet Med. 2013 Mar;30(3):267-75. doi: 10.1111/dme.12039. PMID: 23075228; PMCID: PMC3593165.
- Lean ME, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, Peters C, Zhyzhneuskaya S, Al-Mrabeh A, Hollingsworth KG, Rodrigues AM, Rehackova L, Adamson AJ, Sniehotta FF, Mathers JC, Ross HM, McIlvenna Y, Stefanetti R, Trenell M, Welsh P, Kean S, Ford I, McConnachie A, Sattar N, Taylor R. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet. 2018 Feb 10;391(10120):541-551. doi: 10.1016/S0140-6736(17)33102-1. Epub 2017 Dec 5. PMID: 29221645.
- Yang Y, Wang L, Liu J, Fu S, Zhou L, Wang Y. Obesity or increased body mass index and the risk of severe outcomes in patients with COVID-19: A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2022 Jan 7;101(1):e28499. doi: 10.1097/MD.0000000000028499. PMID: 35029905; PMCID: PMC8735775.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Practicing diabetes specialisation