
CME INDIA Presentation by Kalyan Kumar Gangopadhyay, Abhirup Banerjee, Binayak Sinha, Nilanjan Sengupta, Biswajit Ghosh Dastidar, Soumik Goswami, Ghanshyam Goyal, Sujoy Majumdar, Ajoy Biswas, Sambit Das, Abhay Sahoo, Nagendra Kumar Singh, Koustubh Chakroborty, Sanjay Chatterjee.
(Department of Endocrinology, Peerless Hospital, CK Birla Hospitals, Department of Endocrinology, NRS Medical College, Department of Endocrinology, Fortis Hospital, AMRI Hospitals, Department of Internal Medicine, Woodlands Multispeciality Hospital, Department of Diabetes, ILS Hospital, Departments of Endocrinology, Apollo Hospitals, Kolkata, West Bengal, Department of Medicine, GD Hospital and Diabetes Institute, Kolkata, West Bengal, Department of Endocrinology, Kalinga Institute of Medical Sciences, KIIT, Bhubaneswar, Odisha, Department of Endocrinology, Apollo Hospitals, Bhubaneswar, Odisha, Diabetes and Heart Research Centre, Dhanbad, Jharkhand, Department of Physical Medicine, Peerless Hospital, Kolkata, West Bengal, Diabetes and Endocrinology, Apollo Hospitals, Kolkata, West Bengal, India.)
First consensus to recognise Soleus push‑up exercise.
(Based on a publication in International Journal of Diabetes and Technology 3(2):p 39-48, Apr–Jun 2024. | DOI: 10.4103/ijdt.ijdt_20_24)
Salient Recommendations are simple to understand and follow.
Is exercise is a boon in type 2 DM?
- Exercise significantly improves metabolic parameters, leading to reductions in weight (1.1 kg), waist circumference (3.2 cm), visceral adipose tissue (30–40 cm²), systolic blood pressure (8–12 mmHg), diastolic blood pressure (5–6 mmHg), HbA1c (0.67%), and low-density lipoprotein (3.87 mg/dL).
- Improvements in insulin sensitivity can be observed within 48 hours of exercise, with effects lasting beyond 72 hours. However, the benefits begin to diminish within 48–96 hours after stopping exercise, highlighting the need for a continuous exercise routine.
- Yoga, as an alternative exercise form, also provides metabolic benefits. A meta-analysis of global studies revealed that yoga can lower systolic blood pressure by 5.8 mmHg, diastolic blood pressure by 4.12 mmHg, heart rate by 6.5 beats per minute, and HbA1c by 0.45%, along with improving lipid profiles.
- Beyond these physical benefits, yoga reduces stress, lowers catecholamine levels, enhances mood, and moderates cardiovascular responses to stress. Several trials in India, including randomized controlled studies, have shown yoga’s positive effects on glycemic control, anthropometric measures, lipid profiles, and autonomic function in patients with Type 2 diabetes.
Guideline recommends these types of exercises
Among the various exercise modalities, aerobic exercises are the most convenient and accessible. For older adults, resistance exercises can help increase lean muscle mass. While all exercise types positively affect glycemia and insulin sensitivity, a combination of aerobic and resistance exercises is superior to either type alone. The four main types of exercise are:
- Aerobic: Continuous rhythmic movements involving large muscle groups, such as walking, cycling, jogging, and swimming.
- Resistance: Exercises that involve adding weight to the body, like push-ups, pull-ups, rowing, and weight lifting.
- Flexibility: Exercises that enhance the full range of movement, such as lower back and hamstring stretching exercises.
- Balancing: Activities that improve balance, including yoga, tai chi, standing on one leg, toe walking, walking sideways, or backward.
Intensity is important
Exercise intensity can be categorized into the following levels:
| Low intensity: You can whistle while exercising, such as during slow walking. |
| Moderate intensity: You can hold a conversation but lack the breath to whistle, like during brisk walking. |
| High intensity: Breathing becomes too heavy to comfortably speak in full sentences, as with running, rowing, or cycling. |
| High-intensity interval exercise: Alternates between periods of intense aerobic activity and recovery. |
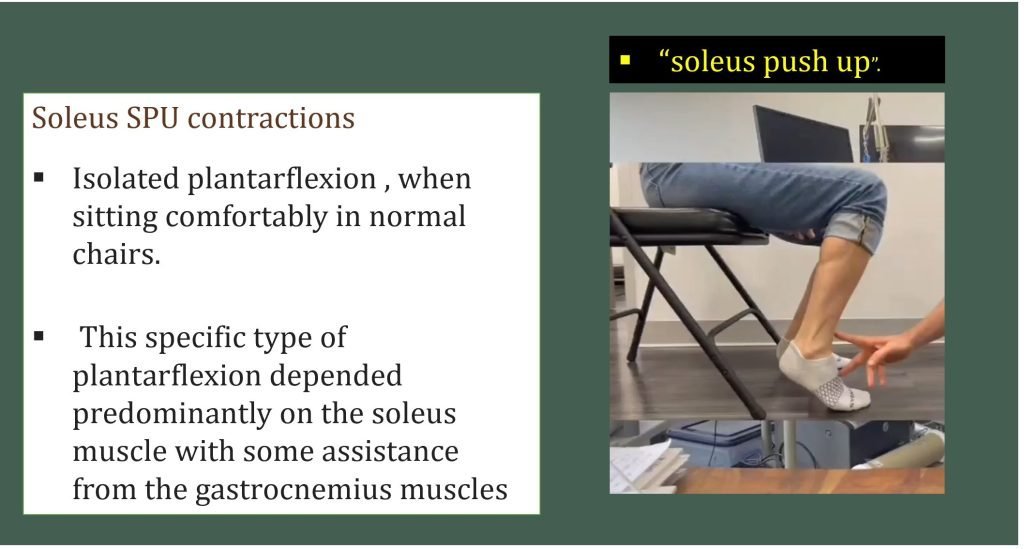
The Guideline recognizes Soleus Push-up
- In today’s world, many people are required to sit for extended periods. The soleus push-up (SPU) can help reduce blood glucose levels.
- Unlike the larger muscles used in activities like walking or running, 88% of the soleus muscle consists of type 1 slow-twitch fibers, which efficiently utilize glucose from the bloodstream without causing fatigue, as they bypass the anaerobic metabolic route. In a unique experiment, performing SPUs continuously for 4 hours led to a 52% reduction in glucose spikes compared to sitting still.
General Exercise Guidelines for Adults with T2DM
| Engage in moderate-intensity exercise for at least 150 minutes per week, spread over a minimum of 3 days, with no more than 2 consecutive days without activity. For younger, physically fit individuals, a shorter duration (at least 75 minutes/week) of high-intensity exercise may suffice. |
| Include resistance training at least twice a week to strengthen muscles. |
| A combination of moderate- and high-intensity exercises is more effective than either type alone. |
| For individuals with chronic conditions or disabilities that limit moderate- or high-intensity exercise, they should participate in as much physical activity as their abilities allow. |
| Incorporate small amounts of physical activity throughout the day to reduce postprandial glucose (PPG) and insulin levels, such as light walking for 3 minutes every 30 minutes of prolonged sitting. |
| Perform flexibility exercises 2–3 times per week to enhance range of motion and prevent conditions like frozen shoulder. |
| Balance training, also 2–3 times per week, is recommended, particularly for older adults. |
Timing of Exercise: Must know Facts
- The timing of exercise can significantly influence its effects on glycemic and lipemic responses to a meal. This is particularly important for Asians and Indians, who tend to experience greater postprandial glucose (PPG) excursions than Caucasians. Among Asians, Indians have higher postprandial insulin spikes compared to Chinese and Malays, even after adjusting for body fat and waist circumference.
- Exercising in a fasted state is more effective at reducing the lipemic effects of a meal, particularly triglycerides, while exercising after a meal helps lower PPG levels. Evidence suggests that South Asians see more significant improvements in postprandial triglycerides and glucose than European Caucasians. A meta-analysis found that post-meal exercise, like a 20-minute walk soon after eating, reduced PPG excursions more effectively than pre-meal exercise. However, the effect diminishes with longer intervals after eating.
- An Indian study compared walking 1500–1600 steps for 15 minutes starting 15 minutes after meals with a one-time daily exercise of 45 minutes (pre-breakfast walking covering 4500–4800 steps). The post-meal exercise group saw significant reductions in HbA1c (−0.7%) and post-lunch glucose levels (−46 mg/dl), while the pre-breakfast exercise group experienced increases in both metrics (+0.3% and +20 mg/dl, respectively).
- But it must be appreciated that Exercising at any time of the day is beneficial:
- Exercise in a fasted state positively impacts lipid levels, particularly by reducing post-meal lipemia.
- Post-meal exercise (0–30 minutes after eating) is more effective at lowering post-meal blood glucose levels than pre-meal exercise.
- Therefore, splitting an exercise routine into two sessions — one in the fasted state and another after meals — can offer optimal benefits.
Exercise Considerations for Those on Oral Hypoglycemic Agents (OHA)
- Patients taking insulin secretagogues, such as sulfonylureas and glinides, have a higher risk of hypoglycemia during exercise, requiring special attention. However, those on medications like metformin, thiazolidinediones, DPP-4 inhibitors, GLP-1 receptor agonists, alpha-glucosidase inhibitors, and SGLT-2 inhibitors typically do not need dose adjustments for exercise.
- Performing a brief high-intensity sprint (10 seconds) before moderate-intensity exercise can help prevent hypoglycemia.
- Exercise should be avoided if there has been a severe hypoglycemic episode in the past 24 hours.
- Glucose Management Before Exercise:
- Glucose < 70 mg/dL: Take 15g of fast-acting carbohydrates (e.g., 15g glucose/sugar). Retest after 15 minutes. Once glucose is >100 mg/dL, low to moderate-intensity exercise is safe. Follow up with slow-acting carbohydrates (e.g., 250 ml milk, 2 biscuits, or 1 piece of fruit).
- Glucose 71–100 mg/dL: Follow the same guidelines as above.
- Glucose 101–270 mg/dL: Exercise is safe, but carry 15g of slow-acting carbohydrates.
- Glucose > 270 mg/dL: If feeling unwell, avoid exercise. If feeling well, proceed with low-intensity exercise, monitor glucose levels, and increase fluid intake.
Exercise in Individuals on Insulin
- Aerobic exercise enhances muscle glucose uptake via both insulin-independent (~2 hours) and insulin-dependent mechanisms (lasting up to ~48 hours with prolonged exercise). Short-duration activities (~20 minutes) with intermittent high intensity, as well as low-intensity exercises lasting 60 minutes or more, can improve insulin sensitivity for at least 24 hours. The improvement in insulin sensitivity correlates with exercise dose, beginning with as little as 400 kcal/week and increasing benefits up to 2500 kcal/week.
- However, longer-duration, high-intensity physical activities can increase the risk of post-exercise hypoglycemia in those using insulin. This risk can be minimized by incorporating a brief maximal-intensity sprint (10 seconds) before or after exercise, adding intermittent high-intensity bouts, or performing resistance exercises immediately before aerobic exercises (if not contraindicated).
- To reduce the risk of exercise-induced nocturnal hypoglycemia, a 20% reduction in daily basal insulin dose, along with reduced prandial bolus insulin and low glycemic index carbohydrate intake after evening exercise, is recommended for those on multiple daily insulin injections. Including a bedtime snack and monitoring glucose overnight can also help mitigate the risk of nocturnal hypoglycemia after exercise.
- In patients using premixed insulin, it may be advisable to reduce the breakfast dose by 20% for daytime exercise and the dinner dose by the same amount for evening exercise. High-intensity activities like sprinting or heavy weightlifting can cause hyperglycemia, which can be managed with a conservative correction dose of insulin (50% of the usual amount) or by incorporating an aerobic cooldown.
- Additionally, insulin should not be injected into the thighs prior to activities involving the thigh muscles, as this could accelerate insulin absorption and raise the risk of hypoglycemia.
Should Patients with T2DM Exercise During Pregnancy?
- Lifestyle management, including physical activity and exercise, is a key component in treating gestational diabetes mellitus. However, before recommending exercise, a thorough clinical examination is essential to rule out any medical contraindications.
- The recommended exercise routine involves 30 minutes of aerobic exercise, such as walking (the safest option), at least 3–4 times per week. The “talk test” is a practical method to measure exercise intensity, which equates to 60%–70% of the heart rate reserve (heart rate reserve = Maximal heart rate (220-age) minus resting heart rate). Exercising with heavy weights should be avoided, while water-based exercise is considered safe.
- Patients should stop exercising immediately if they experience symptoms such as vaginal bleeding, abdominal pain, painful contractions, amniotic fluid leakage, breathlessness, chest pain, headache, muscle weakness affecting balance, or calf swelling.
- Exercise during pregnancy provides numerous benefits to both mother and fetus.
- A routine of 30 minutes of aerobic exercise, 3–4 times a week, is recommended, with the “talk test” as a guide for intensity.
Exercise Recommendations for Older Adults with Type 2 Diabetes (T2DM)
- Assess the individual’s frailty, age-related disabilities, and comorbidities. Tailor exercise programs based on their physical environment, support system, and available resources.
- A well-rounded exercise program should combine:
- Resistance training to maintain muscle strength and physical function.
- Flexibility exercises to preserve joint range of motion.
- Balance exercises to reduce the risk of falls. Initially, balance training should be closely supervised, starting with simpler postures.
- Aerobic activity: Aim for 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic exercise per week.
- A gradual build-up of activity levels is recommended, with breaks as needed.
| Reduce sedentary time: Any physical activity is better than none. |
| Aerobic activity: 150 minutes of moderate or 75 minutes of vigorous aerobic activity weekly. |
| Resistance training: Maintain muscle strength and function. |
| Balance exercises: Essential to prevent falls. |
Should Patients with Type 2 Diabetes (T2DM) and Ischaemic Heart Disease (IHD) Exercise?
- Although cardiovascular disease (CVD) is the leading cause of death in India, many individuals, including those with CVD, remain physically inactive. In patients with ischaemic heart disease (IHD), the benefits of regular exercise far outweigh the risks. Exercise-based cardiac rehabilitation in IHD patients, particularly those recovering from myocardial infarction or revascularization, has been shown to reduce cardiovascular mortality by 26% and hospital admissions by 18%.
- Patients with IHD who do not exhibit high-risk features (as outlined in clinical guidelines) are considered low-risk for exercise-induced adverse events. A clinical evaluation, focusing on the presence of inducible ischemia, can help guide the exercise regimen. Yoga and balance exercises are generally safe for individuals with IHD.
- For those with mild-to-moderate heart failure (HF), exercise training improves exercise capacity and quality of life. Ideally, a supervised cardiac rehabilitation program should be initiated, with non-supervised home-based sessions added gradually.
Exercise Recommendations for Patients with IHD and/or HF:
| 1. IHD: If no high-risk features are present, all activities are generally safe. Initially, supervised exercise programs are ideal, with yoga and balance exercises encouraged. |
| 2. Exertional Angina: Ensure the heart rate remains at least 10 beats per minute below the threshold that induces angina during exercise. |
| 3. Post-Myocardial Infarction: Begin with low-intensity supervised exercise programs. Both aerobic and resistance exercises are allowed. |
| 4. Heart Failure (HF): Avoid exercise if there is hypotension, uncontrolled hypertension at rest or during exercise, or worsening HF symptoms. Aim for low-to-moderate intensity exercise, avoiding activities that cause a significant rise in heart rate. |
Exercise in Patients with Type 2 Diabetes (T2DM) and Retinopathy
- Diabetic retinopathy is a key microvascular complication of diabetes. Regular exercise helps reduce both macrovascular and microvascular complications of diabetes, including retinopathy.
- However, retrospective data suggests that 5%–10% of vitreous hemorrhages may be linked to vigorous exercise. Therefore, exercise routines should be tailored based on the severity of retinopathy. It is recommended to undergo an ophthalmological screening before starting an exercise regimen.
- Recommendations- Exercise for Patients with Retinopathy
- Regular screening for retinopathy is essential, especially before prescribing high-intensity exercise.
- There is no risk from physical activity in cases of mild retinopathy.
- For moderate nonproliferative retinopathy, avoid activities that significantly elevate blood pressure, such as powerlifting and overhead lifting.
Exercise for Patients with Nephropathy
| During the microalbuminuria stage, all types of physical activities can be performed. |
| In cases of overt nephropathy, exercise should begin at low intensity and be gradually increased over time. |
| For patients with end-stage renal disease (ESRD), supervised moderate physical activity during dialysis sessions can help improve physical functioning, reduce depression, and enhance health-related quality of life. |
Exercise in Patients with Neuropathy
- Peripheral Neuropathy: Use appropriate footwear, such as shoes with silica gel midsoles and polyester or blended socks (avoid pure cotton). Focus on non-weight-bearing exercises like cycling, swimming, or seated exercises.
- Local Foot Deformity: Prioritize non-weight-bearing exercises to reduce plantar pressure and protect the feet.
- Autonomic Neuropathy (AN): Avoid exercises that involve rapid postural or directional changes.
- Exercise Environment: Avoid exercising in hot environments and prioritize adequate hydration. Take precautions to prevent postural hypotension. For those with cardiac autonomic neuropathy, seek specialist advice before beginning an exercise routine.
Exercise in Patients with Foot Ulcer
- Aerobic Exercise: Focus on non-weight-bearing exercises, such as seated exercises or upper limb activities. Avoid brisk walking if there are unhealed ulcers.
- Resistance Exercise: Avoid weight-bearing and isometric exercises involving the lower limbs, particularly if there is an ischemic component.
- Flexibility Exercise: These can be performed, provided weight-bearing is avoided on the affected limb (e.g., shoulder flexibility exercises).
Exercise in Patients with Arthritis and Type 2 Diabetes
- Arthropathies such as adhesive capsulitis (frozen shoulder), osteoarthritis, and rheumatoid arthritis are frequently associated with Type 2 diabetes. Physical activity is a key intervention that can positively address the impairments related to aging, arthropathy, and T2DM. The ideal exercise plan should include a mix of different exercise modalities, but some key points must be considered along with guidance on when to stop or modify exercise routines:
- Shoulder mobilization exercises to prevent frozen shoulder.
- Quadriceps and hamstring strengthening exercises for lower limb support.
- Increasing grip size of tools, utensils, and cookware to prevent trigger finger.
- Avoiding high-impact activities that stress the joints.
- Wearing appropriate footwear with a maximum half-inch heel to reduce forefoot pressure.
- Ideally, individuals with arthropathy should be assessed by a specialist in Physical Medicine and Rehabilitation for personalized exercise recommendations.
- Guidance on Adjusting Exercise Routines:
- Mild-to-moderate joint pain: If pain persists for more than 2 hours after exercise, stop for 1–2 days, reduce the intensity, and focus on other joints (e.g., if knee pain, work on the upper body).
- Moderate-to-severe joint pain: Switch to low-impact exercises that place less stress on the joints, such as swimming or underwater walking/exercises.
- Recommendation – Exercise for Patients with Arthritis
| Incorporate a combination of aerobic and resistance exercises. |
| Include flexibility exercises to prevent joint stiffness (e.g., for frozen shoulder). |
| Add balance exercises to reduce the risk of falls. |
| Encourage low-impact exercises like swimming and underwater walking to protect the joints. |
CME INDIA Learning Points
| 1. Exercise as a Pillar of Diabetes Management: Exercise plays a crucial role in managing Type 2 diabetes, but there is limited guidance tailored specifically for Indian patients. |
| 2. Gap in Current Guidelines: While general exercise recommendations for diabetes exist, they often lack specific guidance on accommodating Indian patients or addressing the unique challenges faced by individuals with co-existing complications like diabetic foot, neuropathy, retinopathy, cardiovascular disease, and diabetes during pregnancy. |
| 3. Comprehensive Search: An extensive literature search was conducted using PubMed and Google Scholar up to February 1, 2024, to develop more inclusive exercise recommendations for Indian patients with Type 2 diabetes. |
| 4. Incorporating the Latest Modalities: The recommendation integrates the latest exercise modalities, taking into account both macrovascular and microvascular complications, and provides individualized exercise advice for different conditions associated with Type 2 diabetes. |
| 5. Addressing Comorbidities: Specific exercise guidelines are provided for patients with diabetic foot, neuropathy, retinopathy, cardiovascular disease, elderly patients, and pregnant women with diabetes, which are often overlooked in existing recommendations. |
| 6. Soleus Exercise Inclusion: This recommendation is one of the first to incorporate advice on soleus exercises, which are often omitted from existing diabetes exercise guidelines. |
| 7. Practicality for Indian Context: The recommendations are tailored to the specific needs of Indian patients with Type 2 diabetes, making them a practical guide for physicians in advising their patients on safe and effective exercise plans. |
CME INDIA Tail Piece
Full text available at journal site.
References:
- Gangopadhyay, Kalyan Kumar; Banerjee, Abhirup; Sinha, Binayak; Sengupta, Nilanjan; Dastidar, Biswajit Ghosh; Goswami, Soumik; Goyal, Ghanshyam; Majumdar, Sujoy; Biswas, Ajoy; Das, Sambit; Sahoo, Abhay; Singh, Nagendra Kumar; Chakroborty, Koustubh; Chatterjee, Sanjay. Exercise in Adult Patients with Type 2 Diabetes: Integrated Diabetes and Endocrine Academy Consensus Statement for Indian Patients. International Journal of Diabetes and Technology 3(2):p 39-48, Apr–Jun 2024. | DOI: 10.4103/ijdt.ijdt_20_24
- Armstrong A, Jungbluth Rodriguez K, Sabag A, Mavros Y, Parker HM, Keating SE, et al. Effect of aerobic exercise on waist circumference in adults with overweight or obesity: A systematic review and meta-analysis. Obes Rev 2022;23:e13446.
- Patil SS, Raghuram N, Singh A, Rajesh SK, Ahmed S, Hongasandra N. A prospective study on type-2 diabetic complications and efficacy of integrated yoga: A pan India 2017. Ann Neurosci 2021;28:21-8.
- Hamilton MT, Hamilton DG, Zderic TW. A potent physiological method to magnify and sustain soleus oxidative metabolism improves glucose and lipid regulation. IScience 2022;25:104869.
- Physical activity and exercise during pregnancy and the postpartum period: ACOG Committee Opinion, Number 804. Obstet Gynecol 2020;135:e178-88.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs