
CME INDIA Case Presentation by Dr. N. K. Singh, Editor CME INDIA, Dr. Prabhat Agarwal, Prof. of Medicine, Agra.
CME INDIA Case Study
“In immunocompetent patients, herpes zoster is generally viewed as a self-limited and localized infection. When atypical involvement occurs, it’s crucial to assess the patient’s immunocompetence status and conduct age-specific screening based on their medical history. Additionally, antiviral therapy should be swiftly started in patients who are at elevated risk.”

Patient Profile
- 58-year-old woman
- Known case of type 2 Diabetes
- On triple therapy: Sitagliptin 100mg,Dapagliflozin 10 mg anf Metformin 1000mg
- No Past history of any significant illness
- No smoking or alcohol misuse
- A house wife
Presentation
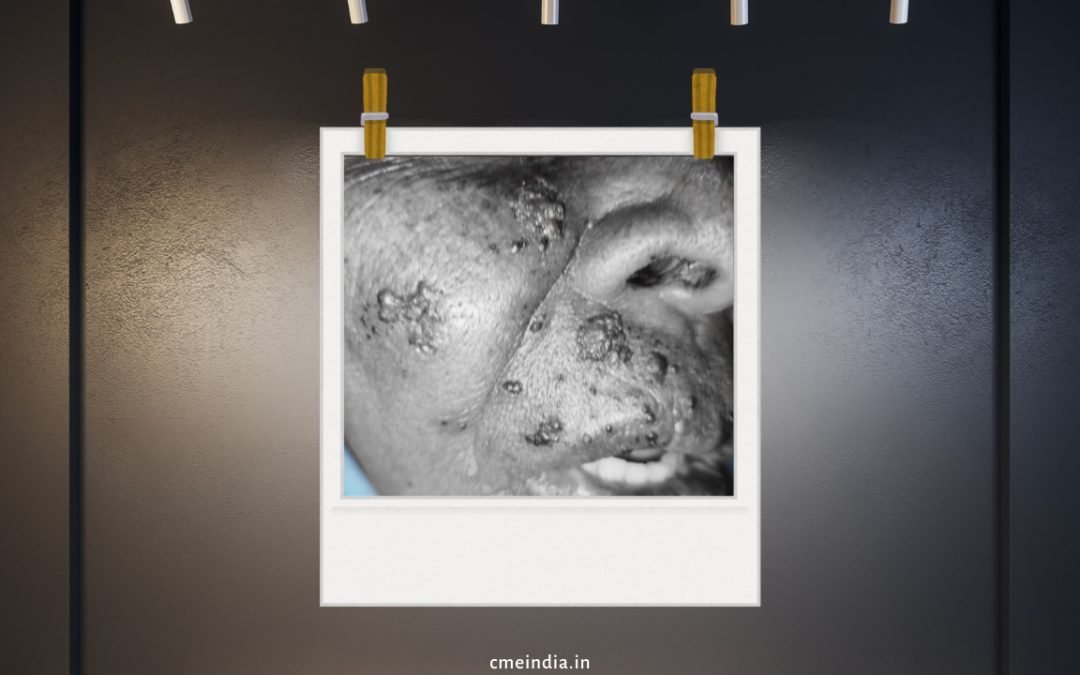
- 5-day history of severe facial skin eruption, swelling, and pain
- She stated that the pain began 5 days before his appointment. She described the pain as a “shooting pain” that radiated to his upper lip and right eye. There was no report of any trigger for the pain.
Examination Findings
- Mild welling of the right face
- Involvement of right eyelid
- Crusted, weeping vesicles over the right side of face/Upper lip
- Erythematous, warm skin—clinically cellulitic
- Hyper-aesthesia over the maxillary (V2) dermatome
- All other cranial nerves normal
- Palpable anterior cervical lymphadenopathy
- Afebrile at presentation, but had documented fevers up to 38°C at home
- No signs of meningism or encephalitis
- No additional lesions on full-body exam
Investigations
- WBC: 6.8 × 10⁹/L, with lymphopenia
- CRP: Mildly elevated at 24 mg/L
- Hb1AC-7.1% PP Sugar-160 mg dl
- Renal function and electrolytes: Normal
- PCR (serum): Positive for Varicella Zoster Virus (VZV) DNA
Differential Diagnosis
- Clinical and microbiological diagnosis: Herpes zoster involving:
- Maxillary (V2)
- Ophthalmic (V1) branches of the trigeminal nerve
- Concern for secondary bacterial infection due to:
- Immunosuppression
- Cellulitic appearance
- Extensive dermal breach
Treatment
- The patient was started on oral valaciclovir with rapid recovery.
Outcome & Follow-Up
- Excellent recovery after 2 months
- Rash cleared well, some scarring
- No postherpetic neuralgia
CME INDIA Discussion
| Yes, herpes zoster (shingles) along the maxillary division (V2) of the trigeminal nerve is uncommon but can occur due to the reactivation of the varicella-zoster virus (VZV). |
| Since the virus remains dormant in the trigeminal ganglion after primary varicella infection, reactivation leads to painful, vesicular eruptions along the affected dermatome. |
| Patients may experience malaise, headache, fever, or burning pain in the maxillary region before the rash appears. |
| Characterized by grouped vesicles on an erythematous base, typically distributed over the cheek, upper lip, lateral nose, and lower eyelid, respecting the midline. |
| Pain and Neuralgia- Can range from mild to severe, with postherpetic neuralgia (PHN) being a significant complication. |
| May affect the hard palate and maxillary gingiva if the palatine nerves are involved. |
| Unlike ophthalmic zoster (V1), eye involvement is rare in V2 zoster unless there is spread. |
| Clinical diagnosis is often sufficient. |
| Tzanck smear, PCR, or direct fluorescent antibody testing can confirm VZV if needed. |
| Antivirals (within 72 hours): Acyclovir, Valacyclovir, or Famciclovir to reduce severity and duration. |
CME INDIA Learning Points
Herpes Zoster in the Maxillary Division (V2)
- Uncommon Location, Significant Impact
- Herpes zoster involving the maxillary (V2) division of the trigeminal nerve is rare but clinically significant.
- Mimics Odontogenic Pain
- In its prodromal phase, V2 herpes zoster may present solely as a toothache, leading to potential misdiagnosis and unnecessary dental procedures.
- Viral Reactivation Can Mimic or Induce Pulpal Pathology
- Varicella-zoster virus reactivation may contribute to pulpal necrosis or apical periodontitis, either directly or through neurogenic inflammation.
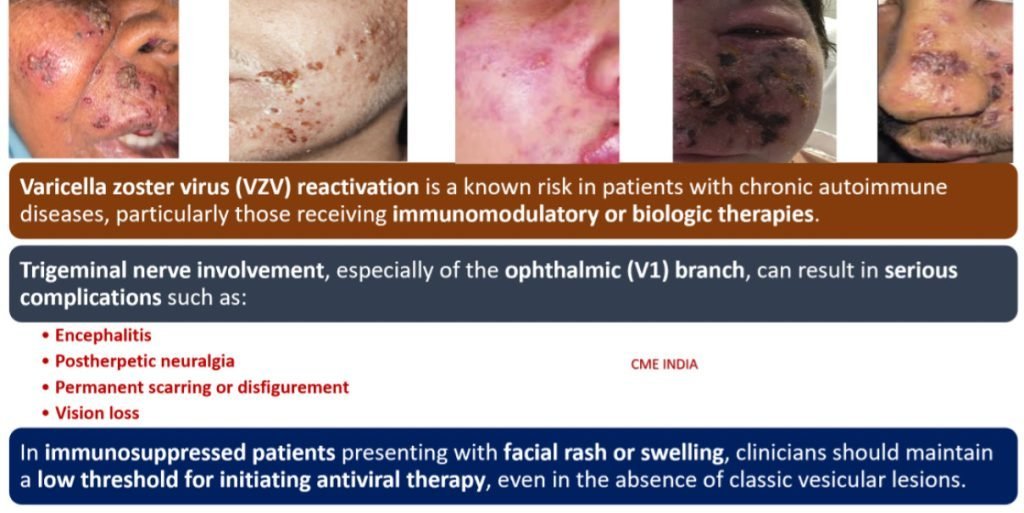
- Classic Vesicular Eruption in the Active Phase
- Progression to the active stage typically reveals a unilateral vesicular rash, midfacial ulceration, crusting, and possible intraoral lesions along the V2 dermatome.
- Endodontic Dilemma
- Endodontists must be aware that herpes zoster may co-exist with or mimic true dental infections; misinterpretation may lead to unnecessary root canal treatment.
- Postherpetic Neuralgia: A Common Sequela
- Postherpetic neuralgia can follow the resolution of active zoster and persist for months, often manifesting as burning or shooting pain in the affected dermatome.
- Delayed Onset, Gradual Resolution
- In the reported case, neuralgia resolved completely by 3 months, with minimal facial scarring – highlighting the importance of early antiviral therapy.
- Neurological Complications Beyond Pain
- Herpes zoster has been increasingly linked with a higher long-term risk of stroke, particularly in older adults.
- Early Antiviral Intervention is Key
- Prompt treatment with antiviral agents (e.g., acyclovir, valacyclovir) reduces viral replication, severity of symptoms, and risk of postherpetic neuralgia.
- Always Consider VZV in Facial Pain Differentials
- In elderly patients with midfacial pain, ulceration, or atypical toothache, herpes zoster should be high on the differential, especially if no dental etiology is evident.
References:
- Paquin R, Susin LF, Welch G, Barnes JB, Stevens MR, Tay FR. Herpes Zoster Involving the Second Division of the Trigeminal Nerve: Case Report and Literature Review. J Endod. 2017 Sep;43(9):1569-1573. doi: 10.1016/j.joen.2017.03.004. Epub 2017 Jun 27. PMID: 28662876.
- Lovell B. Trigeminal herpes zoster: early recognition and treatment are crucial. BMJ Case Rep. 2015 Mar 20;2015:bcr2014208673. doi: 10.1136/bcr-2014-208673. PMID: 25795749; PMCID: PMC4369019.
- Rebecca Paquin, Lisiane F. Susin, Garrett Welch, Jonathan B. Barnes, Mark R. Stevens, Franklin R. Tay,Herpes Zoster Involving the Second Division of the Trigeminal Nerve: Case Report and Literature Review,Journal of Endodontics,Volume 43, Issue 9,2017,Pages 1569-1573,ISSN 0099-2399,https://doi.org/10.1016/j.joen.2017.03.004
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs