
CME INDIA Presentation by Dr. Pratap P. Jethwani, M.D (Medicine) FRCP (Glasgow), Post graduate diploma in diabetes (Cardiff, U.K),Fellow- RSSDI, Fellow-DiabetesIndia, Ex Tutor- Leicester University, U.K, National Joint Secretary – RSSDI, Past Chairman – Gujarat State Chapter of RSSDI, Past Advisory Council Member- ACP India Chapter.
The Somogyi effect refers to a pattern
- The Somogyi effect refers to a pattern where nocturnal hypoglycemia (low blood sugar during the night) triggers a counter-regulatory hormonal surge—primarily involving cortisol and growth hormone—that results in elevated morning blood glucose (morning hyperglycemia).
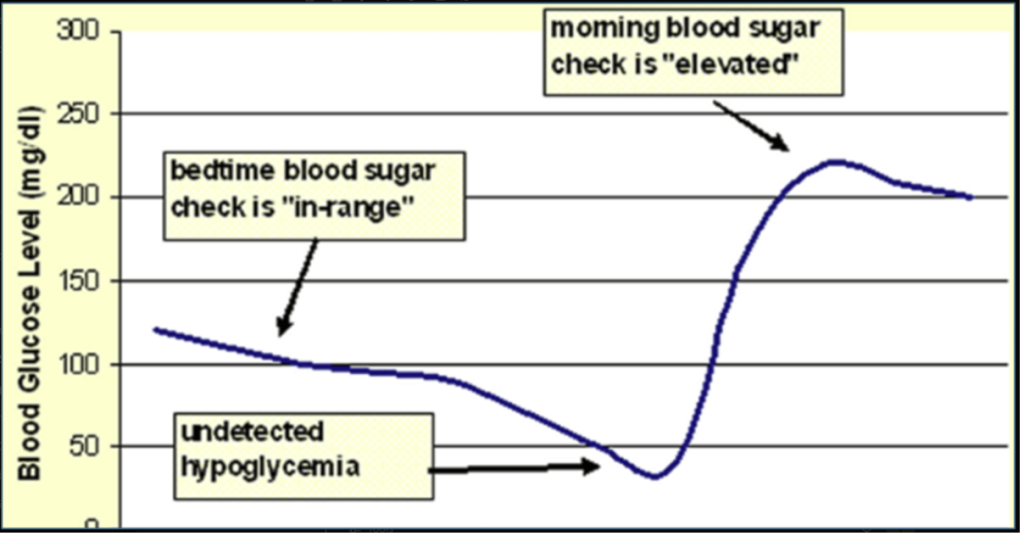
Understanding this Graph
This pattern is described as the Somogyi phenomenon, first described by Michael Somogyi in 1938. Cryer PE. Hypoglycemia, functional brain failure, and brain death. J Clin Invest. 2007;117(4):868–870. DOI: 10.1172/JCI31773
Explanation of the graph:
- X-axis (horizontal): Time (overnight period).
- Y-axis (vertical): Blood glucose level (mg/dL).
- The blue curve shows the patient’s blood glucose trend overnight.
- Bedtime blood sugar “in-range”:
- Before sleep, glucose levels are normal (~100 mg/dL) and may give a false sense of good control.
- Undetected nocturnal hypoglycemia:
- During the night (around 2–3 AM), blood glucose falls steeply and drops below 50 mg/dL — hypoglycemia goes unnoticed if not checked.
- Counter-regulatory response:
- The body reacts by releasing hormones (e.g., glucagon, cortisol, growth hormone, catecholamines) that cause hepatic glucose production, leading to rebound hyperglycemia.
- Morning blood sugar “elevated:”
- Despite a good bedtime reading, the patient wakes up with high fasting glucose (~200 mg/dL)due to this rebound.
Clinical relevance:
- This graph underscores the importance of checking 3 AM blood sugars when fasting hyperglycemia is observed.
- Differentiating Somogyi effect from Dawn phenomenon (which is due to early morning rise in hormones but without preceding hypoglycemia) is key for adjusting therapy.
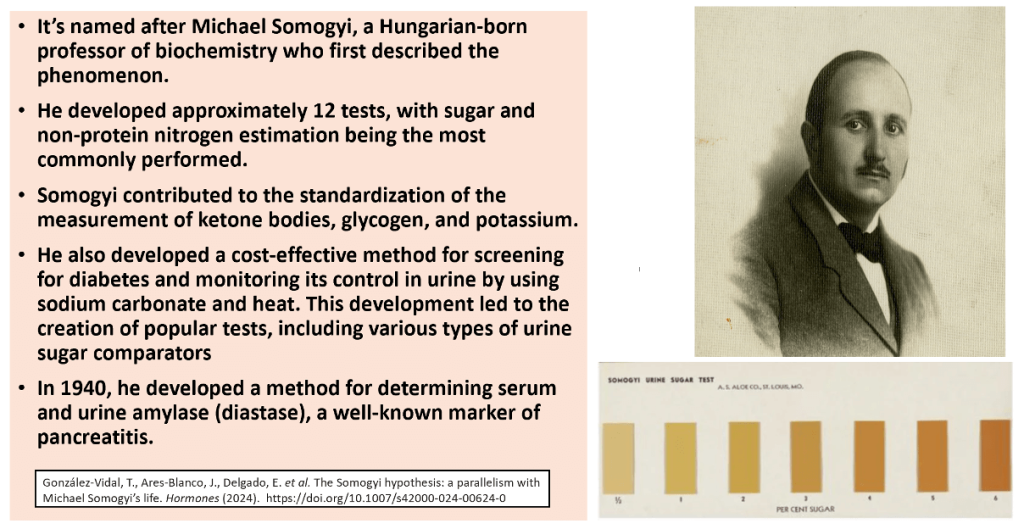
This seminal 1959 paper by Michael Somogy
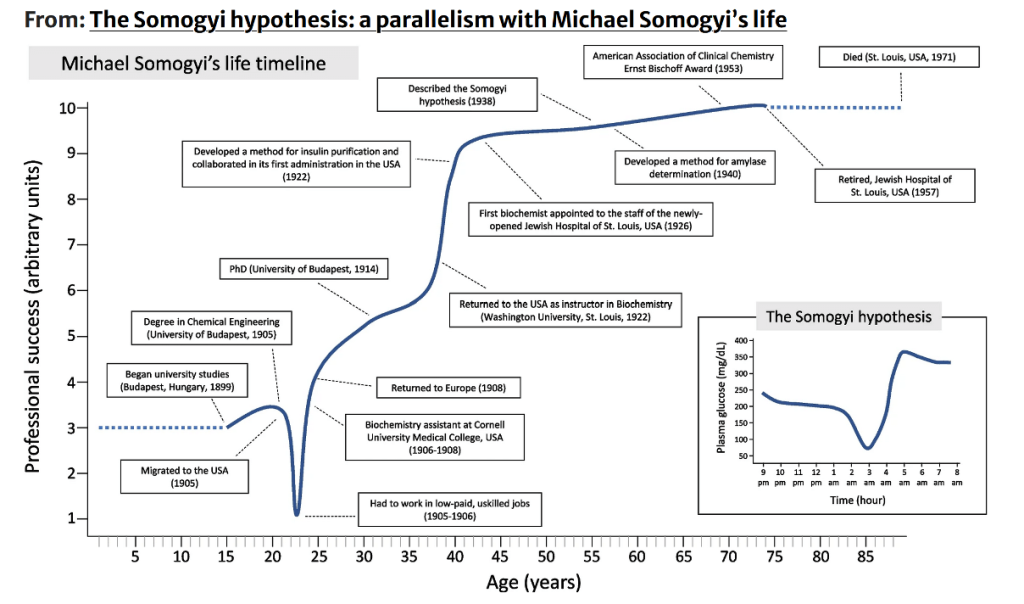
Courtesy: González-Vidal, T., Ares-Blanco, J., Delgado, E. et al. The Somogyi hypothesis: a parallelism with Michael Somogyi’s life. Hormones (2024). (https://doi.org/10.1007/s42000-024-00624-0)
Must be considered:These results were based only on Urine Glucose estimation during different times of day and they correlated episodes of low urine Glucose followed by episodes of high Urine Glucose and based on that they suggested this hypothesis of rebound hyperglycemia in response to hypoglycemia
So basically somgyi effect is based on this primitive method of Urine Glucose estimation.
- Laboratory records of patients receiving substantial insulin doses reveal a recurring pattern: fluctuations in blood glucose and glycosuria, with spikes in hyperglycemia consistently following hypoglycemic episodes—even mild or asymptomatic ones. This establishes a clear The cause-and-effect relationship between hypoglycemia and subsequent hyperglycemia, highlighting the paradox that excess insulin can, in fact, lead to hyperglycemia.
- Experimental evidence, supported by our own studies, explains this phenomenon: hypoglycemia triggers an accelerated release of adrenal-pituitary hormones that raise blood sugar levels.
- When clinicians mistakenly respond to this insulin-induced hyperglycemia by further increasing insulin doses—assuming the hyperglycemia reflects insufficient insulin—the result is a worsening diabetic state, characterized by extreme swings in glycosuria, rising glucose peaks, ketonuria, and increasingly severe recurrent hypoglycemic episodes.
In search of the Somogyi Effect
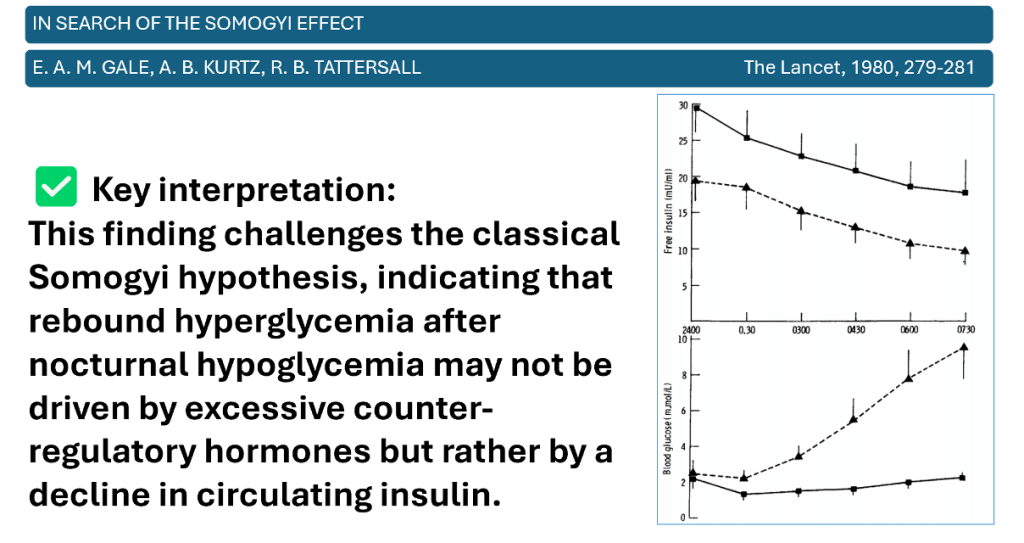
- In a study of 15 patients with 17 episodes of asymptomatic, untreated nocturnal hypoglycemia (blood glucose <2 mmol/L between 11 PM and 3 AM), fasting blood glucose at 7 AM varied widely (0.7–17 mmol/L). Notably, 6 patients exhibited apparent rebound hyperglycemia (>7 mmol/L), but their levels of growth hormone, cortisol, and glucagon were not higher than those without significant recovery of glucose.
- Importantly, there was a strong inverse correlation (r = –0.996, p < 0.001) between blood glucose and free insulin levels, suggesting that when morning hyperglycemia occurred, it was primarily due to relative insulin deficiency later in the night, rather than a counter-regulatory hormonal surge.”
- When glucagon secretion is suppressed, recovery from hypoglycemia is significantly impaired during adrenergic blockade and does not occur at all if epinephrine is also absent. This indicates that glucagon is the primary hormone responsible for recovery from insulin-induced hypoglycemia in nondiabetic individuals.
- Recovery fails only when both glucagon and epinephrine are absent.
- In contrast, acute cortisol or growth hormone release is not essential for this recovery, and neither sympathetic neural norepinephrine release nor glucose autoregulation is strong enough to restore glucose levels. Therefore, these mechanisms are not required to explain recovery from insulin-induced hypoglycemia
Study by Havlin, Carolyn & Cryer, Philip. (1987)
- Blood glucose concentrations were routinely measured using a glucometer (Ames, Miles, Elkhart, IN) at 0700, 1100, 1600, 2100, and 0300 hours by research nurses monitoring patients enrolled in the Diabetes Registry program at the Washington University Diabetes Research and Training Center.
- The findings indicate that nocturnal hypoglycemia does not commonly lead to significant morning or daytime hyperglycemia in patients with diabetes mellitus while they are on their usual therapeutic regimens
Does the Somogyi effect truly exist?
- In clinical practice, many diabetes specialists- endocrinologists still believe in this phenomenon and they do not intensify treatment, particulalry insulin therapy in patients having morning hyperglycemia suspecting the presence of this phenomenon but
- Does the Somogyi effect truly exist? Continuous glucose monitoring systems can help track blood glucose changes overnight and can help identify somogyi phenomenon in a true manner
Somogyi phenomenon reconsidered (Diabetologia 2005):
- A study using continuous glucose monitoring in 262 patients with T1DM found:
- Morning glucose after nocturnal hypoglycemia was >5 mmol/L lower than after nights without hypoglycemia.
- No evidence for rebound hyperglycemia following nocturnal hypoglycemia.
- Risk of nocturnal hypoglycemia progressively increased as morning glucose levels decreased.
- Conclusion:
This study challenges the classic Somogyi hypothesis—suggesting that nocturnal hypoglycemia does not commonly result in morning hyperglycemia in real-life conditions.
This Study concluded it is Fiction
- One 2013 study data provide no support for the Somogyi effect. Fasting capillary glucose < 5 mmol/L suggests a high probability of asymptomatic nocturnal hypoglycaemia, whereas bedtime readings > 10 mmol/L should prompt confident overnight insulin adjustment.(Ref-5)
Takeishi S, et al. 2016
- Pre-breakfast glucose levels were significantly lower in patients with nocturnal hypoglycemia (p=0.03). The magnitude of glucose rise after breakfast was significantly greater in these patients (p=0.047), suggesting that marked pre- to post-breakfast increases may help predict nocturnal hypoglycemia.(Ref-6)
Furukawa F, Nishimura R, Sakamoto M, et al,2022
- In a retrospective CGM analysis of 2,600 insulin-treated type 2 diabetes patients, morning fasting glucose was lower after nights with nocturnal hypoglycemia (P<0.001).
Fasting glucose <3.9 mmol/L in the morning predicted 100% risk of nocturnal hypoglycemia, whereas fasting glucose >9.6 mmol/L was associated with no risk of nocturnal hypoglycemia, refuting the Somogyi effect. - With the advent of continuous glucose monitoring systems (CGMs), the Somogyi effect proved to be rare or absent in most studies in the recent decades.
- Fasting glucose levels after nights with nocturnal hypoglycemia were lower than those after nights without nocturnal hypoglycemia, and the more severe the nocturnal hypoglycemia was, the lower the fasting glucose levels were.
Take Home Message
The Somogyi effect: Fact or fiction?
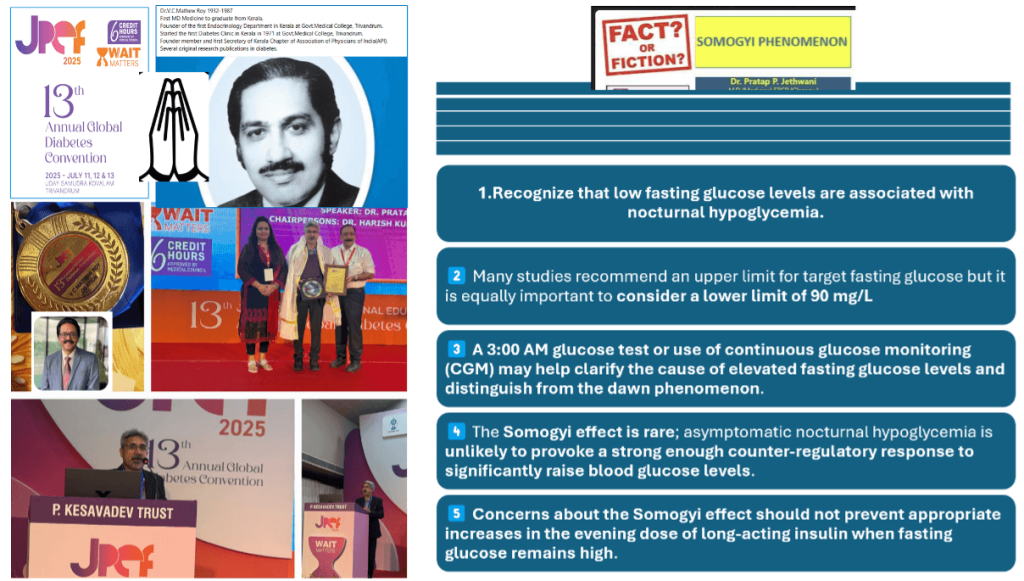
| 1. Recognize that low fasting glucose levels are associated with nocturnal hypoglycemia. |
| 2. Many studies recommend an upper limit for target fasting glucose but it is equally important to consider a lower limit of 5 mmol/L. |
| 3. A 3:00 AM glucose test or use of continuous glucose monitoring (CGM) may help clarify the cause of elevated fasting glucose levels and distinguish from the dawn phenomenon. |
| 4. The Somogyi effect is rare; asymptomatic nocturnal hypoglycemia is unlikely to provoke a strong enough counter-regulatory response to significantly raise blood glucose levels. |
| 5. Concerns about the Somogyi effect should not prevent appropriate increases in the evening dose of long-acting insulin when fasting glucose remains high. |
References:
- Cryer PE. Hypoglycemia, functional brain failure, and brain death. J Clin Invest. 2007;117(4):868–870. DOI: 10.1172/JCI31773
- González-Vidal, T., Ares-Blanco, J., Delgado, E. et al. The Somogyi hypothesis: a parallelism with Michael Somogyi’s life. Hormones (2024). https://doi.org/10.1007/s42000-024-00624-0
- Cryer PE: Glucose counterregulation in man. Diabetes 1981;30: 261-264
- Havlin, Carolyn & Cryer, Philip. (1987). Nocturnal Hypoglycemia Does Not Commonly Result in Major Morning Hyperglycemia in Patients With Diabetes Mellitus. Diabetes care. 10. 141-7. 10.2337/diacare.10.2.141.
- Choudhary P, Davies C, Emery CJ, Heller SR. Do high fasting glucose levels suggest nocturnal hypoglycaemia? The Somogyi effect—more fiction than fact? Diabet Med. 2013;30:914–917.
- Takeishi S, et al. Major increases between pre- and post-breakfast glucose levels may predict nocturnal hypoglycemia in type 2 diabetes. Intern Med. 2016;55:2933–2938.
- Furukawa F, Nishimura R, Sakamoto M, et al. Confirmation of the Absence of Somogyi Effect in Patients with Type 2 Diabetes by Retrospective Continuous Glucose Monitoring Systems. International Journal of Endocrinology. 2022;2022:Article ID 6599379, 5 pages. https://doi.org/10.1155/2022/6599379
- Choudhary P, Heller S. The Somogyi effect: Fact or fiction? Diabetes & Primary Care. https://diabetesonthenet.com/wp-content/uploads/dpc10-6pg335-340-1.pdf
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Somogyi effect has been a controversy since 2022 study on 2500 + patients on insulin.
Common explanation of early morning hyperglycemia :
1. Dawn Phenomenon
Definition: The dawn phenomenon refers to a natural rise in blood glucose that occurs between about 3 a.m. and 8 a.m.
Cause: This is due to the early-morning secretion of hormones such as cortisol, growth hormone, glucagon, and epinephrine, which stimulate the liver to release more glucose into the bloodstream.
It is considered the most common cause of early morning hyperglycemia in people with both type 1 and type 2 diabetes.
2. Insufficient Overnight Insulin
This occurs when insulin levels drop too low during the night, either because the dose of basal (long-acting) insulin is too small, it is timed incorrectly, or an insulin pump is not set high enough overnight.As the effect of insulin wanes, blood sugar rises unopposed, leading to high glucose readings in the morning.
Inadequate insulin at bedtime or early timing of long-acting insulin injection.
3. Lifestyle and Medication Factors like bedtime carbohydrate consumption
Eating high-carbohydrate snacks late at night can contribute to higher morning blood sugars, especially if insulin or medication does not fully match the increase.
Missed Insulin or Medications can be another factor.
4. Insulin Resistance
Mechanism: Increased insulin resistance in the early morning, partly due to the body’s hormonal cycles, may exacerbate the rise in blood glucose.
It was indeed good knowledge churning review of topic. It is always important to know 3 AM sugar values if patient develops early morning hyperglycemia.
Controversy is well taken by Dr. Pratap.
With use of CGMS we are now better equipped to know such events in real life evidences and it reduces our judgemental errors.