
CME INDIA Presentation by Dr. Parimal Swamy, Consultant Physician, JH & RC | Professor (Medicine), HIDS | Director, Apollo Asthma & Diabetes Care Centre | Compiled for CME India.
(Based on a presentation at Hello Academia 2026, Nagpur)
Abstract
Type 2 diabetes therapeutics is in the middle of its most crowded developmental phase since the incretin era began. More than thirty molecules are now in active development across at least a dozen distinct mechanisms, from oral and injectable incretin agonists to glucokinase activators, mitochondrial modulators and muscle-targeted adrenergic agents. This article summarizes the current pipeline, the mechanistic logic that links each class to a clinical phenotype, and the most recent 2026 trial readouts that are reshaping practice.
1. Why the Pipeline Has Suddenly Widened
For nearly two decades, glucose-lowering pharmacology added new classes one at a time — DPP-4 inhibitors, then SGLT2 inhibitors, then injectable GLP-1 receptor agonists. What is happening now is different in kind, not just in degree. A single hormone family, the incretins, has become a scaffold onto which additional biology is being layered: GIP agonism or antagonism, glucagon agonism, amylin pathway engagement, and even IGF-1 signalling are being combined with GLP-1 in the same molecule. At the same time, entirely non-incretin strategies — glucokinase activation, mitochondrial bioenergetics, and muscle-targeted adrenergic signalling — are advancing in parallel, offering options for patients and phenotypes that do not respond well to incretin-based therapy alone.
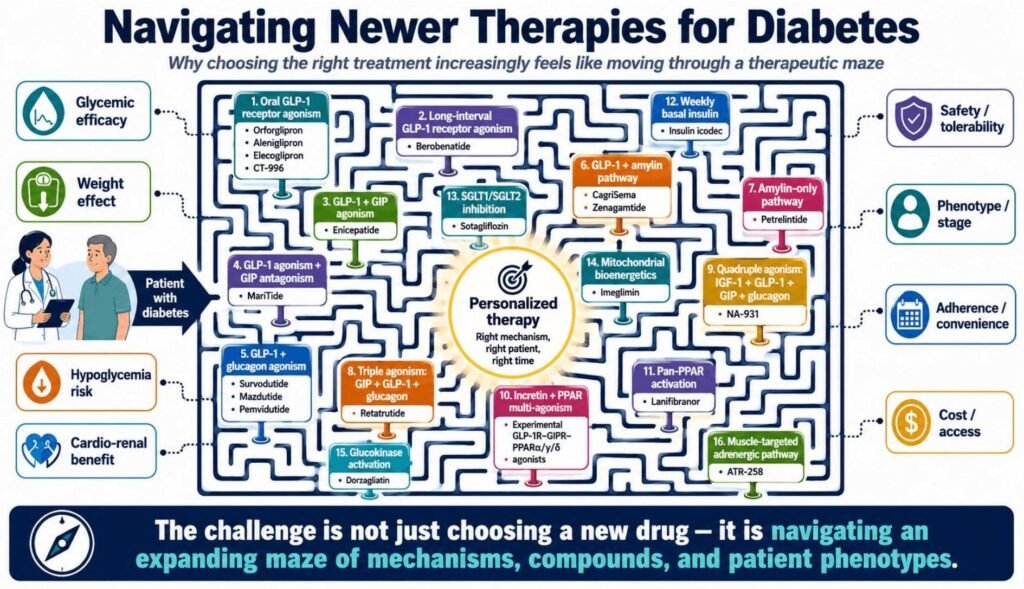
Figure 1. The expanding therapeutic maze — choosing a new agent today means navigating mechanism, phenotype, safety, and cost simultaneously.
A Simple Way to Remember the Pathways
Each mechanism nudges a different metabolic bottleneck. GLP-1 and amylin reduce food intake and blunt the post-meal glucose excursion. GIP agonism amplifies incretin biology, whereas GIP antagonism appears to prevent fat storage — a paradox that is still being worked out mechanistically. Glucagon agonism, when balanced against GLP-1, adds liver-fat oxidation and energy-expenditure effects rather than simply raising glucose. Glucokinase activation restores defective glucose sensing in the beta cell and liver. Mitochondrial agents improve cellular energy handling, and muscle-targeted adrenergic therapy tries to make skeletal muscle behave as though it has just exercised.
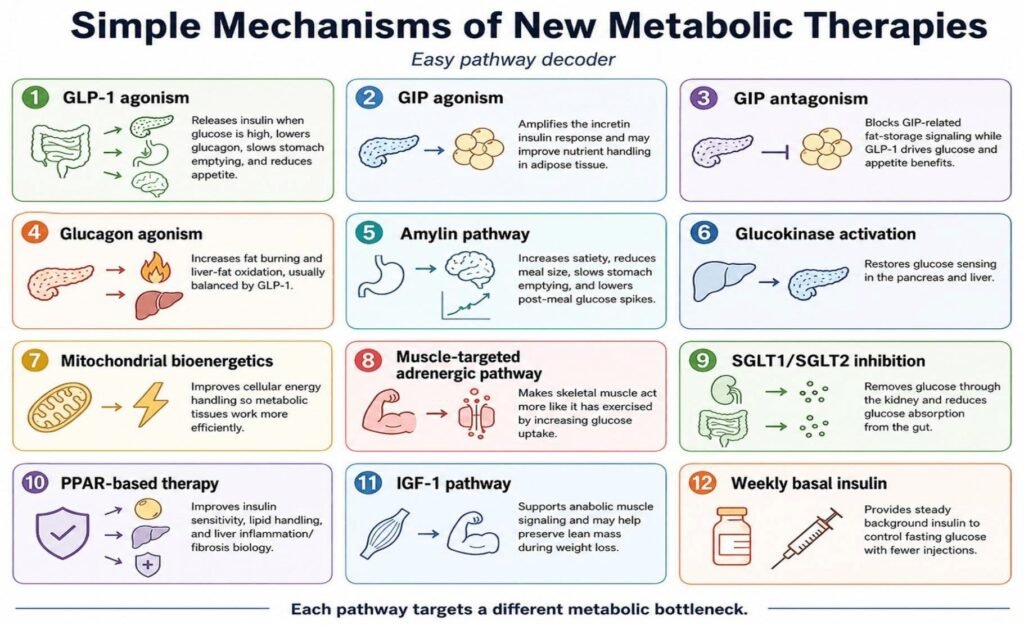
Figure 2. A pathway decoder — each mechanism targets a distinct metabolic bottleneck.
2. Development Stage: What “Phase 3” Actually Means for the Clinic
It is worth restating a point that is easy to lose in headline-driven coverage: a drug in Phase 1 is experimental, a drug in Phase 2 is promising but unproven, and a drug in Phase 3 is late-stage but still not available until regulators approve it. Phase 1 asks whether a molecule is safe; Phase 2 asks whether it works; Phase 3 asks whether it is good enough for approval at scale; and Phase 4 — post-marketing surveillance — asks what happens in real-world practice, after the controlled-trial population gives way to the messier reality of comorbidity and non-adherence. Clinicians should calibrate enthusiasm accordingly when patients bring in pipeline drug names from social media.
This distinction matters more in 2026 than it did five years ago, because the volume of press-released topline data has outpaced peer-reviewed publication. A molecule can generate weeks of trade-press coverage on the strength of a company statement, while the full dataset, safety tabulation, and regulatory verdict lag by months. For patient counselling, a useful habit is to separate three questions before discussing any pipeline agent: has it completed Phase 3, has it been published in a peer-reviewed journal, and has any regulator actually approved it for the indication being discussed. Many of the molecules named in this article satisfy the first criterion but not the third.
3. The Current Pipeline at a Glance
The following mechanism-based classification captures the major programs currently in clinical development or newly approved, current as of mid-2026:
| Mechanism / Class | Representative Compound(s) and Status |
| Oral GLP-1 receptor agonism | Foundayo (orforglipron) — FDA approved 1 Apr 2026; aleniglipron, elecoglipron — Phase 2; CT-996 — Phase 1 |
| Long-interval GLP-1 agonism | Berobenatide — once-monthly SC, Phase 2b |
| GLP-1 + GIP dual agonism | Enicepatide — Phase 2 |
| GLP-1 agonism + GIP antagonism | MariTide (maridebart cafraglutide) — Phase 3, monthly SC |
| GLP-1 + glucagon dual agonism | Survodutide, Pemvidutide — Phase 3; Mazdutide — approved in China |
| GLP-1 + amylin pathway | CagriSema — Phase 3 (REDEFINE/REIMAGINE programs); Zenagamtide (amycretin) — Phase 3 planned |
| Amylin-only pathway | Petrelintide — Phase 3 planned |
| Triple agonism (GIP+GLP-1+glucagon) | Retatrutide — Phase 3 (TRIUMPH/TRANSCEND programs) |
| Quadruple agonism (IGF-1+GLP-1+GIP+glucagon) | NA-931 — early clinical |
| Weekly basal insulin | Insulin icodec (Awiqli) — approved in selected regions |
| Dual SGLT1/SGLT2 inhibition | Sotagliflozin — approved for cardiorenal indications in selected regions |
| Mitochondrial bioenergetics | Imeglimin — approved in Japan and India |
| Glucokinase activation | Dorzagliatin — approved in China |
| Muscle-targeted adrenergic pathway | ATR-258 — Phase 1 |
| Pan-PPAR activation | Lanifibranor — Phase 3, MASH-focused |
| Discontinued (cautionary example) | Danuglipron — Pfizer halted development on tolerability grounds |
4. Efficacy Landscape: Glucose-Lowering vs Weight-Loss Potential
No single agent dominates on every axis, and the relative ranking is shifting month to month as 2026 Phase 3 data mature. Retatrutide, the triple GIP/GLP-1/glucagon agonist, currently sits at the top of both efficacy axes. In the TRIUMPH-1 obesity trial (topline 21 May 2026), the 12 mg dose produced a mean weight loss of roughly 28% at 80 weeks in patients without diabetes, extending to close to 30% by 104 weeks in a severe-obesity extension cohort — among the largest sustained pharmacological weight-loss effects reported in any trial to date. In patients with type 2 diabetes, the TRANSCEND-T2D-1 trial (published in The Lancet, March 2026) showed HbA1c reductions of 1.7–2.0 percentage points with 11.5–16.8% weight loss over 40 weeks, alongside a distinctive dysesthesia signal in a minority of patients that clinicians should watch for.
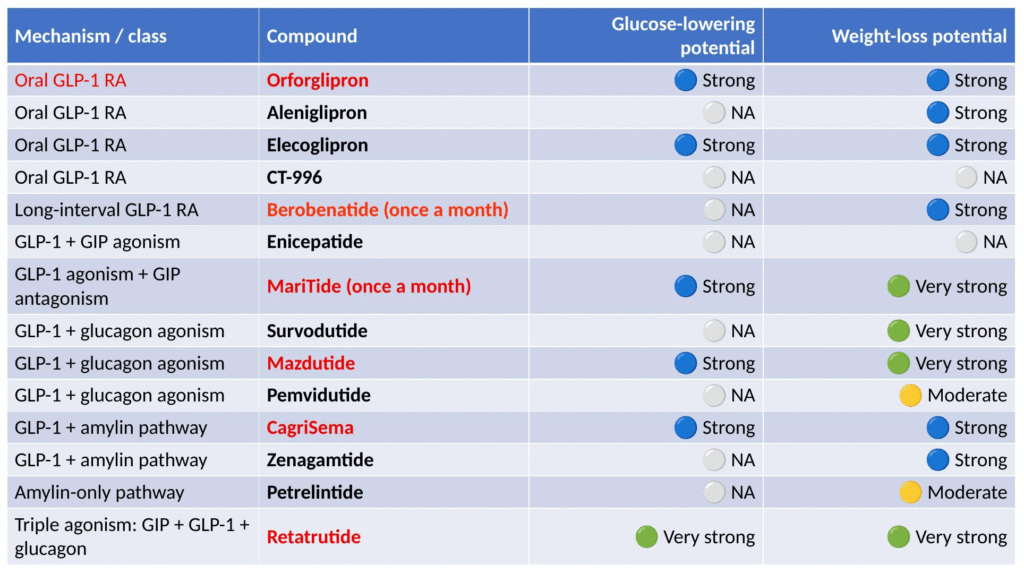
Figure 3. Comparative glucose-lowering and weight-loss potential across the pipeline (qualitative synthesis).
CagriSema, MariTide, Mazdutide, elecoglipron and orforglipron form the next tier. CagriSema’s REIMAGINE 1–3 program, presented at ADA 2026 and published simultaneously in The Lancet and The Lancet Diabetes & Endocrinology, showed superior HbA1c reduction and weight loss compared with semaglutide alone across multiple type 2 diabetes populations, including basal-insulin-treated patients in whom add-on CagriSema lowered HbA1c from 8.8% to 6.5% with up to 12% weight loss and no severe hypoglycemia. In the obesity-only REDEFINE program, CagriSema produced roughly 20–23% weight loss versus placebo, and the company filed for weight-management approval with the FDA in December 2025. Orforglipron, the first oral GLP-1 receptor agonist to reach approval, was cleared by the FDA on 1 April 2026 as Foundayo for chronic weight management, based on the ATTAIN-1 and ATTAIN-2 trials (72-week mean weight loss of approximately 12% at the highest dose); its type 2 diabetes filing, built on the ACHIEVE program, is expected later in 2026, with ACHIEVE-3 showing superior HbA1c and weight reduction versus oral semaglutide, at the cost of somewhat higher gastrointestinal discontinuation.
5. Matching Mechanism to Phenotype
The clinically useful question is rarely “which drug is strongest” in the abstract; it is “which mechanism fits this patient.” A simple phenotype-driven framework, drawn from the CME India teaching deck, is reproduced below.
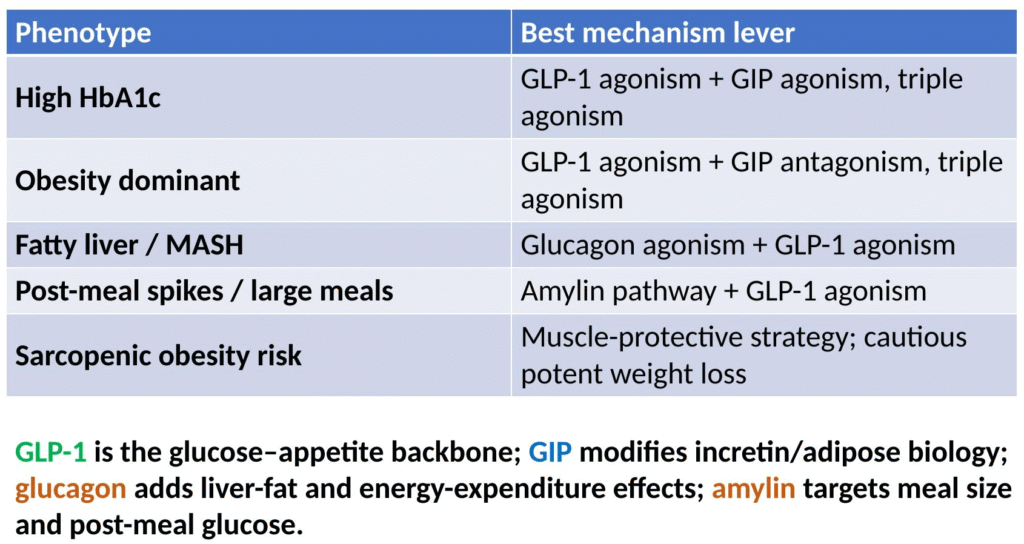
Figure 4. Phenotype-to-mechanism mapping for individualized selection.
- High HbA1c dominant — GLP-1 + GIP agonism, or triple agonism (retatrutide, CagriSema).
- Obesity dominant — GLP-1 agonism combined with GIP antagonism or triple agonism (MariTide, retatrutide, survodutide).
- Fatty liver / MASH phenotype — glucagon agonism plus GLP-1 agonism (survodutide, mazdutide, pemvidutide).
- Post-meal glucose spikes / large-meal eating pattern — amylin pathway plus GLP-1 (CagriSema, zenagamtide, petrelintide).
- Sarcopenic-obesity risk — a muscle-protective strategy and cautious pursuit of potent weight loss, with attention to protein intake and resistance training alongside pharmacotherapy.
- Injection-averse patients — oral agents (orforglipron/Foundayo, aleniglipron, elecoglipron, CT-996).
- Poor-adherence phenotype — long-interval dosing (berobenatide monthly, MariTide monthly, insulin icodec weekly).
It is worth remembering that insulin — unglamorous as it may seem next to triple agonists — remains clinically relevant, particularly for patients with advanced beta-cell failure or acute decompensation for whom incretin-based options alone are insufficient. In routine Indian outpatient practice, the phenotype framework above is best used as a starting filter rather than a rigid algorithm: most patients present with overlapping features — an obese patient with fatty liver and post-meal spikes, for instance — and the choice of agent should weigh cost, injection tolerance, local drug availability, and comorbidity burden alongside the mechanistic fit.
6. Beyond Glucose-Lowering: Type 1 Diabetes and Regenerative Approaches
A parallel and conceptually distinct research effort is asking whether type 1 diabetes can move from lifelong hormone replacement toward disease modification or cure. The maturity map for this field separates what is available or approved today from what remains an active research frontier.
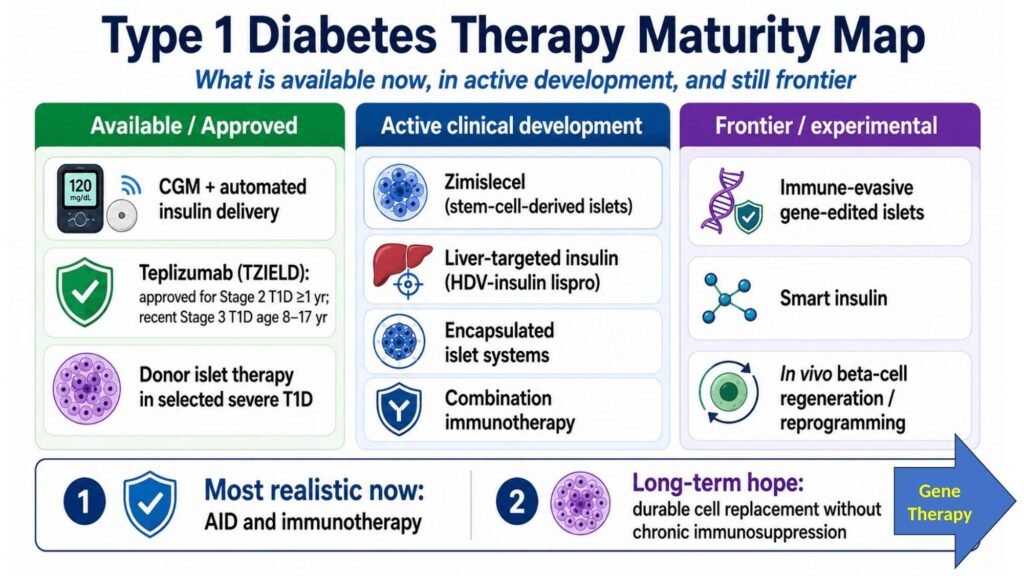
Figure 5. Type 1 diabetes therapy maturity map — from CGM-augmented insulin delivery to immune-gene-edited islets.
At the near-term end, automated insulin delivery with CGM integration and selected immunotherapy (teplizumab, approved for stage 2 T1D delay in some regions) represent realistic, deployable options. Donor islet therapy and encapsulated islet-cell systems are in active clinical development. At the far end of the maturity map, gene-edited immune-evasive islets and in vivo beta-cell regeneration or reprogramming remain early-stage and experimental. The take-home message for T2D and T1D gene-therapy approaches differs: in type 2 disease, gene-therapy concepts mostly aim to modify metabolic signalling pathways, whereas in type 1 disease the emphasis is on protecting or restoring beta-cell mass and function. Stem-cell-derived islet replacement currently looks more realistic in the near term than durable gene-based beta-cell regeneration.
7. Practical Synthesis: What Is Realistic Today
For a working diabetologist counselling patients in 2026, the honest answer is that most of this pipeline is not yet prescribable, and enthusiasm should be proportionate to phase. A practical roadmap, distinguishing what is approved, what is best-in-class by trial data, and what remains a realistic interpretation for now, is summarized below.
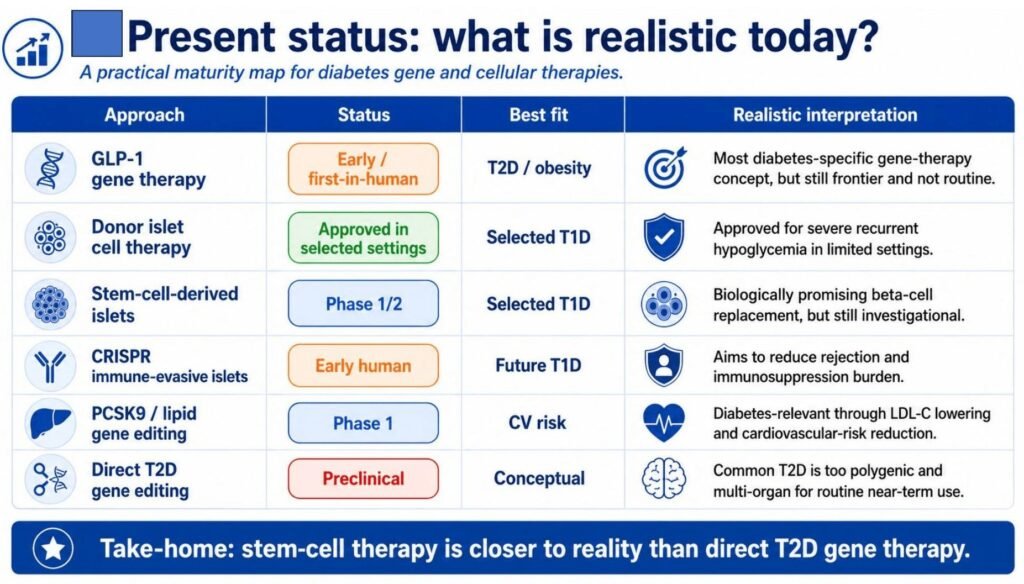
Figure 6. A practical maturity roadmap for diabetes gene- and cell-based therapy — present status.
Among agents already usable in Indian practice or likely to be available soon, imeglimin (approved in Japan and India) offers a low-hypoglycemia-risk option well suited to beta-cell dysfunction and metabolic-fatigue phenotypes, while sotagliflozin’s cardiorenal indication extends the SGLT-inhibitor story beyond glycemic control alone. Weekly basal insulin (icodec) addresses adherence but does not itself produce weight loss and needs careful up-titration counselling — a stepwise initiation, monitoring and intensification pathway, rather than a fixed starting dose, is now the recommended approach for weekly basal insulin regimens.
8. Clinical Pearls for CME India Readers
- Do not equate “in the news” with “available” — confirm regulatory status (Phase, approved-region, or discontinued) before counselling patients who ask about a pipeline drug by name.
- Match mechanism to phenotype rather than chasing the single most potent agent — a fatty-liver-dominant patient may benefit more from a glucagon-GLP-1 dual agonist than from the highest-weight-loss option on the market.
- Watch for class-specific signals as new agents reach practice: dysesthesia has emerged as a retatrutide-specific finding at high cumulative exposure; gastrointestinal tolerability remains the dominant limiting factor across the entire GLP-1-based class, oral or injectable.
- Sarcopenic obesity deserves proactive attention — pair potent incretin-based weight loss with protein intake and resistance training, and consider muscle-sparing mechanisms (ATR-258, NA-931) as they mature.
- Insulin has not been replaced — it remains essential for patients with advanced beta-cell failure, and weekly basal insulin formulations are improving adherence without eliminating the need for structured initiation and monitoring.
A Note on Access for Indian Practice
Most of the agents discussed here will reach Indian pharmacies later, and at different price points, than their US or European launch dates — a pattern already visible with existing GLP-1 receptor agonists. Two practical implications follow. First, Indian-approved or Indian-manufactured options already on the shelf — imeglimin, sotagliflozin, and the existing GLP-1/SGLT2 combinations — should remain the default workhorses while newer multi-agonists work through pricing and access negotiations. Second, when a patient can access one of the newer agents through import, trial participation, or overseas travel, the phenotype-matching logic in Section 5 is still the right filter to apply, rather than defaulting to whichever molecule is best-known from international media coverage.
9. Conclusion
The diabetes and obesity pipeline in mid-2026 is unusually dense, and the pace of Phase 3 readouts — orforglipron’s approval as Foundayo, retatrutide’s TRIUMPH and TRANSCEND results, and CagriSema’s REIMAGINE and REDEFINE programs — means the practical map will keep shifting through the rest of the year. For Indian clinicians, the enduring task is unchanged: translate mechanism into phenotype-appropriate choice, stay skeptical of phase-inappropriate enthusiasm, and keep foundational therapies — metformin, SGLT2 inhibitors, and insulin — in view even as the incretin-based ceiling keeps rising.
References:
1. Eli Lilly and Company. Lilly’s oral GLP-1, orforglipron, is successful in third Phase 3 trial, triggering global regulatory submissions for the treatment of obesity [press release]. Indianapolis: Eli Lilly; 2025 Aug.
2. US Food and Drug Administration. Foundayo (orforglipron) approval letter, NDA 220934. Silver Spring (MD): FDA; 2026 Apr 1.
3. Giorgino F, et al. ACHIEVE-3: oral orforglipron versus oral semaglutide in type 2 diabetes on metformin. Lancet. 2026 Mar 21.
4. ACHIEVE-5 investigators. Once-daily oral orforglipron added to basal insulin in type 2 diabetes. JAMA. 2026 Jun 7.
5. Eli Lilly and Company. TRIUMPH-1: topline Phase 3 results of retatrutide in adults with obesity or overweight [press release]. Indianapolis: Eli Lilly; 2026 May 21.
6. TRANSCEND-T2D-1 investigators. Retatrutide in type 2 diabetes inadequately controlled by diet and exercise: a phase 3 randomised trial. Lancet. 2026 Mar 19.
7. Novo Nordisk A/S. CagriSema demonstrated significant reduction in HbA1c and weight across the REIMAGINE 1-3 phase 3 programme [press release]. Bagsværd: Novo Nordisk; 2026 Jun 7.
8. REDEFINE 1 investigators. CagriSema 2.4 mg/2.4 mg in adults with overweight or obesity: a phase 3 randomised trial. N Engl J Med. 2025.
9. Pfizer Inc. Update on oral GLP-1 receptor agonist danuglipron development programme [press release]. New York: Pfizer; 2023 Dec.
10. Drugs.com. CagriSema (cagrilintide and semaglutide): development status and FDA filing timeline. Updated 2026 Feb 23.
11. Swamy P. Future Glucose-Lowering Therapy in the Pipeline [CME teaching deck]. CME India / RSSDI educational archive; 2026.
For educational use by registered medical practitioners. This summary does not replace full prescribing information; verify current regulatory status in your jurisdiction before clinical application.
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs