
CME INDIA Presentation by CME INDIA Team.
This medical research article presents a large-scale, real-world study investigating the incidence of urogenital infections among over 15,000 type-2 diabetes patients across India. The findings reveal that patients using SGLT2 inhibitors face a significantly higher risk of both urinary and genital tract infections compared to those on other medications. Notably, the data suggests that combining SGLT2i with DPP4 inhibitors is associated with a lower incidence of these infections, potentially offering a protective effect. The study identifies specific high-risk groups, including females, elderly patients, and those with obesity, who are more susceptible to these side effects. By examining diverse geographical regions, the authors provide essential evidence to help clinicians balance the cardio-renal benefits of these drugs against infection risks. Ultimately, the research emphasizes the importance of personalized therapeutic strategies and routine monitoring for diabetic patients in the Indian clinical landscape.
SGLT2 Inhibitors, UTI/Genital Infection Risk, and the “DPP4i Signal” from Real-World India
Based on: Singh N.K., Singh A.K., Gupta A. et al. Real-world evidence of urinary tract infections and genital tract infections with sodium-glucose cotransporter-2 inhibitors alone or in combination with dipeptidyl peptidase-4 inhibitors in individuals with type-2 diabetes mellitus in India. BMC Endocrine Disorders, 2026. DOI: 10.1186/s12902-026-02304-z. The article is listed as accepted on 29 April 2026 and is currently available as an article-in-press version.
Why this study matters?
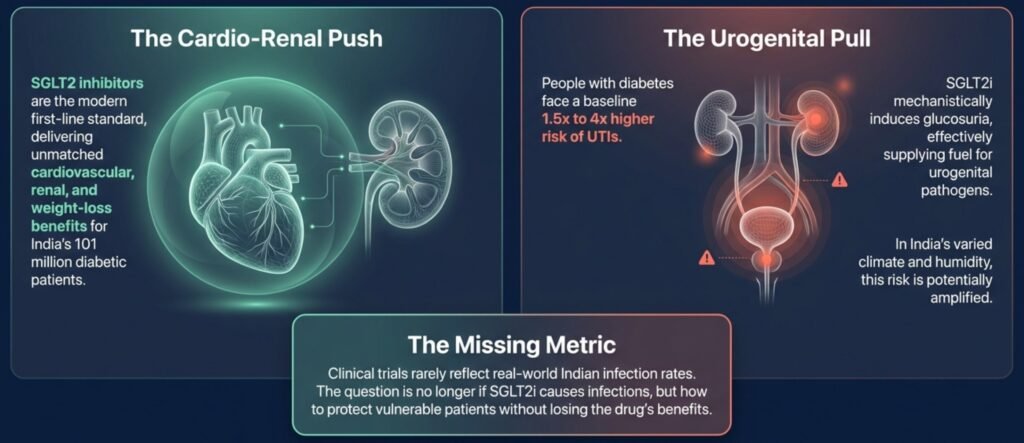
SGLT2 inhibitors have changed the therapeutic landscape of type 2 diabetes. Their value is no longer limited to glucose lowering; they are now widely used because of their cardiovascular, renal, metabolic, and weight-related benefits. In routine Indian diabetes practice, dapagliflozin and empagliflozin are now frequently prescribed not only for glycaemic control but also for cardiorenal protection. However, the same mechanism that makes these drugs effective—promoting urinary glucose excretion—also creates a biological setting that may favour genital mycotic infections and, in some patients, urinary tract infections.
For Indian physicians, this issue is clinically important. India has a large population living with type 2 diabetes, and the study background notes an estimated Indian diabetes prevalence of 11.4%, affecting around 101 million individuals. SGLT2 inhibitors and DPP4 inhibitors are also commonly combined in Indian prescriptions because both have low hypoglycaemia risk and are convenient oral agents. Yet robust Indian real-world data on urogenital infection risk with these combinations has been limited. This multicentre study directly addresses that gap by examining urinary tract infections and genital tract infections among patients with type 2 diabetes across India.
Study design in brief
This was a large, multicentre, cross-sectional, real-world observational study conducted across primary and secondary healthcare facilities in India. Adult patients aged 18 years or above with type 2 diabetes were included if they were attending routine consultations and had been receiving at least one oral antidiabetic drug for at least one month before enrolment. Pregnant or lactating women, patients below 18 years, those who declined consent, and acutely unwell patients requiring emergency care were excluded.
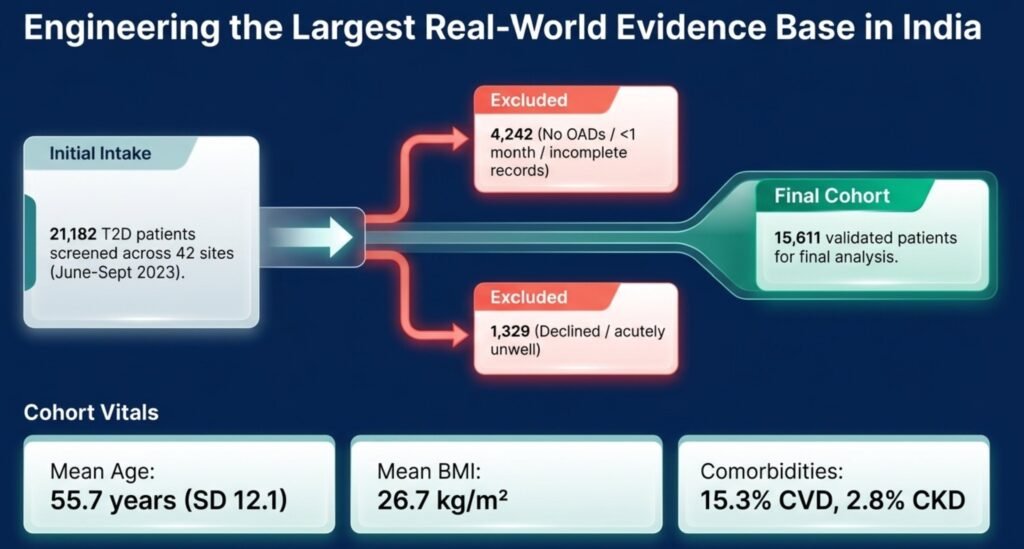
The recruitment window was from 15 June to 30 September 2023. Initially, 21,182 individuals with type 2 diabetes were screened. After exclusion of patients who did not meet medication-duration criteria, had incomplete records, declined consent, or were acutely unwell, 15,611 patients were included in the final analysis. The study flow diagram shows this transition from screened participants to the final analytic cohort.
Data were extracted from routine clinical records, including prescriptions, laboratory records, radiological data, and other relevant investigations. Importantly, urinary tract infection diagnosis was not based only on patient self-report. It required physician documentation in routine records and was based on clinical history, examination, and relevant investigations such as urine microscopy and/or culture where available. Genital tract infection diagnosis was established by symptoms, local examination, and investigations when performed. This gives the dataset practical real-world credibility, although the authors also acknowledge that microbiological confirmation was not standardised across all sites.
Primary and secondary outcomes
The primary outcome was the incidence of urogenital infection, defined as urinary tract infection and/or genital tract infection, during the six months before study enrolment. The study also aimed to determine whether SGLT2 inhibitor use was associated with a statistically significant increase in urogenital infections, and whether this risk differed when SGLT2 inhibitors were used with or without DPP4 inhibitors.
Secondary outcomes included variation in infection incidence according to geography, sex, age group, BMI category, and comorbidities such as chronic kidney disease and cardiovascular disease. Statistical analysis included chi-square testing for categorical comparisons, logistic regression for adjusted odds, and propensity score matching to reduce measured confounding across treatment groups.
Who were the patients?
The final cohort included 15,611 patients with type 2 diabetes from 42 sites across India, representing diverse geographical regions. The mean age was 55.7 years, and the mean BMI was 26.7 kg/m². Men constituted 55.8% of the cohort and women 44.2%. Most patients did not have chronic kidney disease or cardiovascular disease recorded as comorbidity; 80% had neither CKD nor CVD.
In terms of BMI profile, 35.9% were in the normal BMI range, 39.8% were overweight, and 21.8% were obese. This is clinically relevant because increasing BMI emerged as one of the important infection-risk signals. Duration of diabetes was also varied: 35.1% had diabetes for 3–10 years, and 27.3% for more than 10 years. This means the study represents a typical Indian outpatient diabetes population, including many patients with long-standing disease and multiple-drug therapy.
Medication exposure was particularly important. All participants were on at least one oral antidiabetic drug among metformin, sulfonylureas, alpha-glucosidase inhibitors, or pioglitazone. The commonest regimens were metformin plus sulfonylurea and metformin alone. Among the newer agents, 73% were on DPP4 inhibitors, 66% were on SGLT2 inhibitors, and 52.2% were receiving both. Dapagliflozin was the most frequently used SGLT2 inhibitor, followed by empagliflozin. Sitagliptin, vildagliptin, linagliptin, and teneligliptin were the DPP4 inhibitors recorded.
Main result: overall urogenital infection burden
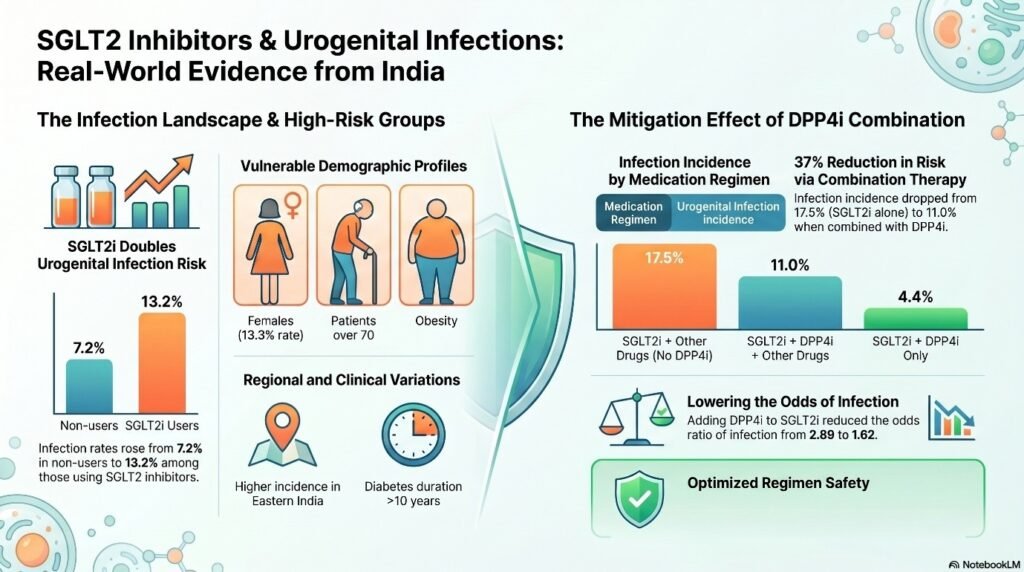
The overall incidence of urogenital infection—UTI and/or GTI—was 11.3%. Separately, genital tract infection occurred in 5.8%, while urinary tract infection occurred in 7.1%. These rates are important for real-world counselling: roughly one in nine patients in this diabetes cohort had a documented urogenital infection in the preceding six months.
Women had significantly higher infection rates than men: 13.3% versus 9.7%. This finding is biologically and clinically plausible. Women with diabetes are already known to have higher UTI susceptibility, and genital infections may also be more frequent when glycosuria, local moisture, and impaired host defence coexist. Older age and obesity also showed higher infection rates. Patients above 70 years had an infection rate of 13.4%, while those with BMI ≥30 kg/m² had a rate of 13.7%.
Comorbid kidney disease also mattered. The reported infection rate in patients with CKD was higher than in those without CKD/CVD. This is clinically important because CKD patients are often candidates for SGLT2 inhibitor therapy because of renal-protective benefits, yet they may also be more vulnerable to infection, dehydration, frailty, and complications if infection is missed.
SGLT2 inhibitor signal: higher infection incidence
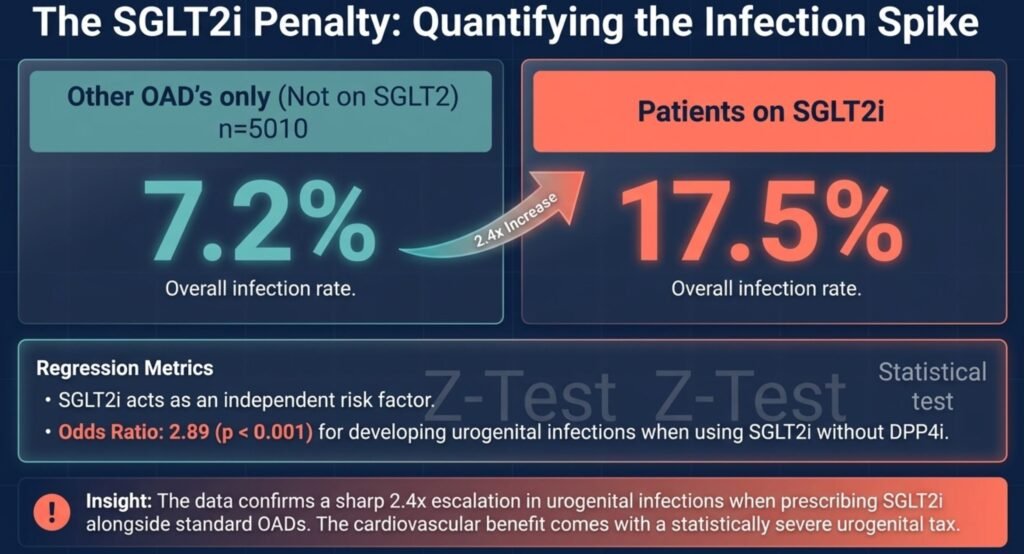
The most direct finding was that patients receiving SGLT2 inhibitors had a significantly higher incidence of urogenital infections than patients not receiving SGLT2 inhibitors. Infection incidence was 13.2% among SGLT2 inhibitor users compared with 7.2% among non-users. The difference was statistically significant.
The same pattern was observed when infections were separated into genital and urinary categories. Genital tract infection was 7.5% in SGLT2 inhibitor users versus 2.3% in non-users. Urinary tract infection was 7.7% in SGLT2 inhibitor users versus 5.4% in non-users. This distinction is important: the genital infection signal was stronger than the UTI signal, which is consistent with much of the broader SGLT2 inhibitor literature, where genital mycotic infection is a more reproducible adverse effect than bacterial UTI.
The study’s Figure 2, a bar chart comparing infection incidence by SGLT2 inhibitor use, visually demonstrates this pattern: urogenital infection, genital infection, and UTI were all higher in SGLT2 inhibitor users than in patients using other oral antidiabetic drugs alone.
The most interesting finding: DPP4i combination may reduce observed infection risk
The most provocative result is not merely that SGLT2 inhibitors were associated with more infections. That is expected and clinically familiar. The novel Indian signal is that patients receiving SGLT2 inhibitors with DPP4 inhibitors had lower observed urogenital infection rates than those receiving SGLT2 inhibitors without DPP4 inhibitors.
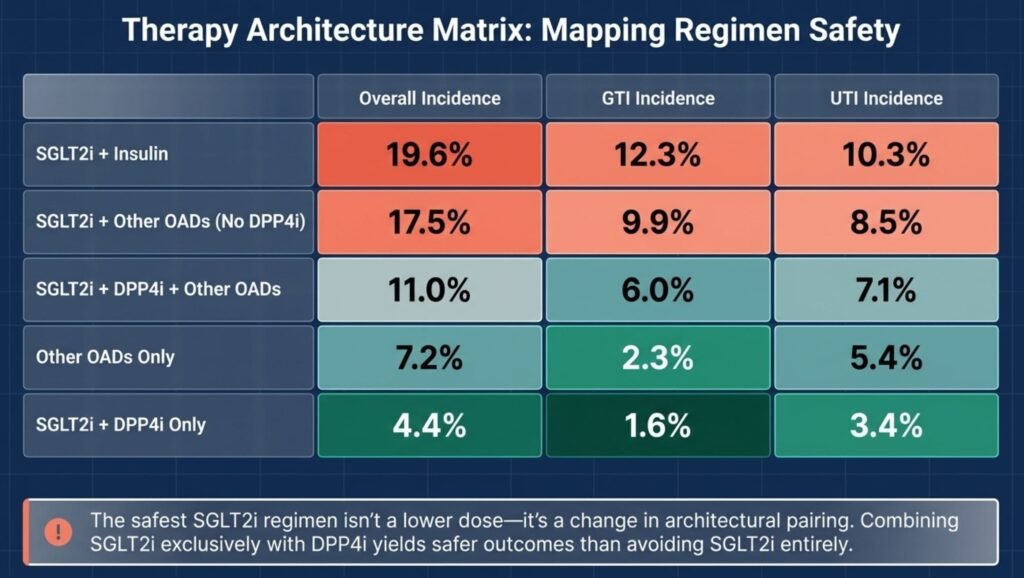
Among patients using SGLT2 inhibitors with other oral antidiabetic drugs but without DPP4 inhibitors, the urogenital infection incidence was 17.5%. When DPP4 inhibitors were added alongside SGLT2 inhibitors and other oral drugs, the incidence decreased to 11.0%. The lowest observed incidence was seen in patients taking SGLT2 inhibitor plus DPP4 inhibitor without other oral antidiabetic drugs, at 4.4%.
This is the key “CME INDIA clinical alert” from the paper. It does not prove that DPP4 inhibitors protect against infections, because this was not a randomised trial. However, the finding generates an important hypothesis: the combination of SGLT2 inhibitor and DPP4 inhibitor may have a more favourable urogenital tolerability profile than SGLT2 inhibitor regimens used in more complex or insulin-associated treatment settings.
One possible explanation is confounding by disease severity. Patients on insulin or multiple oral agents may have longer-standing diabetes, poorer glycaemic control, more complications, or higher baseline infection risk. The group receiving only SGLT2 inhibitor plus DPP4 inhibitor may represent a metabolically different population: possibly earlier disease, fewer comorbidities, better preserved renal function, lower treatment complexity, or better adherence to counselling. Therefore, this finding must be interpreted as an association, not a therapeutic guarantee.
Adjusted analysis: risk persists, but DPP4i attenuates the odds
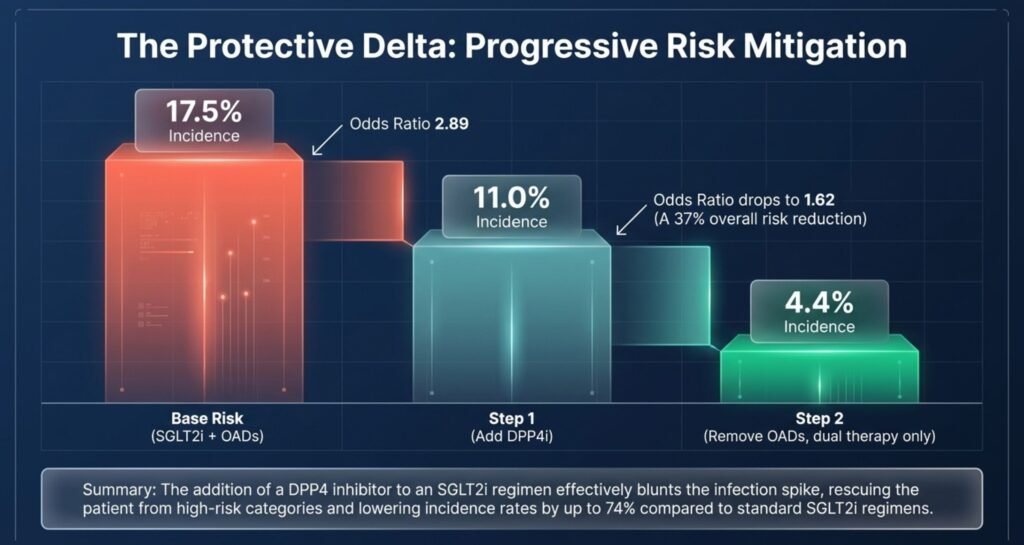
The regression analysis further supports the signal. SGLT2 inhibitor use was associated with increased odds of urogenital infection, with an odds ratio of 2.89. When DPP4 inhibitor was added, the odds were lower, reported as 1.62. The model had 61% accuracy, and the authors used adjustment approaches including logistic regression and propensity score matching to address measured confounding such as age, sex, BMI, CKD, and CVD.
For clinicians, the practical interpretation is balanced. SGLT2 inhibitor therapy remains associated with higher infection risk in this Indian real-world population, but the magnitude of risk appears lower when DPP4 inhibitors are part of the regimen. This should not be overinterpreted as proof of a protective pharmacological effect, but it should encourage further prospective research.
Which patients need extra caution?
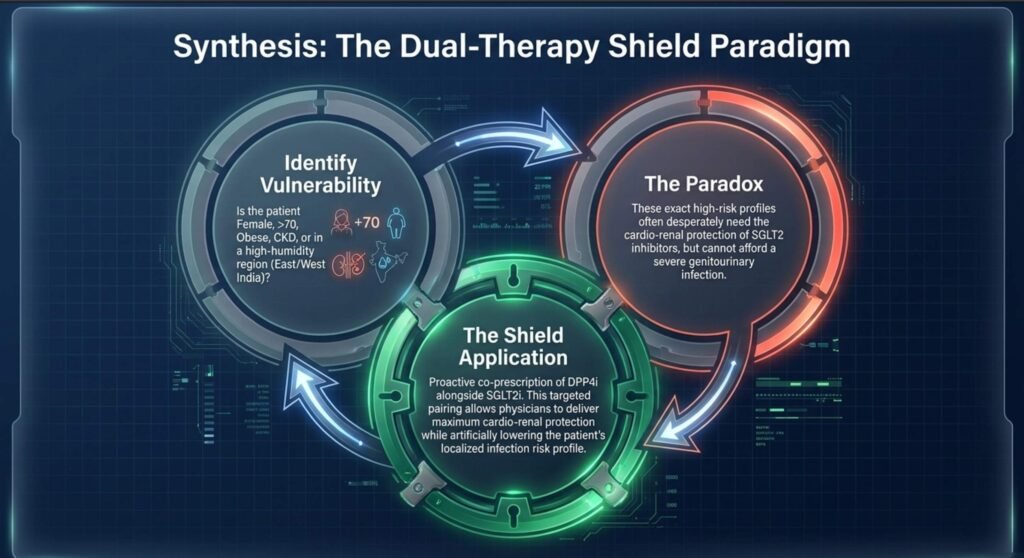
This study identifies several high-risk clinical profiles. Women had higher urogenital infection rates than men. Older patients, especially those above 70 years, had higher infection rates. Obesity was associated with increased infection incidence, with BMI ≥30 kg/m² showing one of the higher rates. CKD also appeared to be associated with greater infection burden. Longer duration of diabetes, particularly more than 10 years, was associated with higher UTI incidence.
From a practice point of view, these findings suggest that before starting SGLT2 inhibitors, Indian physicians should assess baseline infection risk. This should include prior history of recurrent UTI, recurrent balanoposthitis, vulvovaginal candidiasis, poor genital hygiene, urinary obstruction, incontinence, postmenopausal status, uncontrolled hyperglycaemia, CKD, frailty, and concomitant insulin use.
The study also showed geographical variation. Infection incidence differed across regions of India, with higher overall rates reported in some regions than others. This may reflect climate, humidity, hygiene practices, healthcare-seeking behaviour, documentation differences, or prescribing patterns. Such regional variation is especially relevant for India, where environmental and socioeconomic conditions differ widely.
What should Indian physicians do differently?
The message is not to avoid SGLT2 inhibitors. These drugs have major cardiorenal advantages and are now central to modern diabetes care. The message is to prescribe them intelligently, counsel proactively, and monitor early.
Patients should be informed about symptoms of genital infection: itching, redness, discharge, local discomfort, dysuria, balanitis, vulvovaginitis, and recurrent irritation. They should also be taught UTI warning symptoms: burning micturition, frequency, urgency, suprapubic discomfort, fever, flank pain, and unexplained deterioration in glycaemic control. In elderly or CKD patients, symptoms may be atypical, so clinicians should maintain a low threshold for urine testing.
Genital hygiene counselling should become a routine part of SGLT2 inhibitor initiation. Patients should be advised on adequate hydration, avoidance of prolonged damp underclothing, timely reporting of symptoms, and avoiding self-medication with inappropriate antibiotics or topical steroid combinations. In men with recurrent balanoposthitis and in women with recurrent vulvovaginal candidiasis, drug continuation should be individualised.
Strengths of the study
The major strength is scale. A cohort of 15,611 patients from 42 Indian sites provides one of the largest real-world datasets on this issue from India. It reflects routine practice, not the controlled environment of randomised trials. This is particularly useful for adverse-event questions, where real-world behaviour, hygiene, climate, comorbidity, and drug combinations matter.
The study also separated UTI and genital tract infection instead of merging them vaguely. It assessed multiple treatment cohorts, including SGLT2 inhibitor users, non-users, SGLT2 inhibitor plus DPP4 inhibitor users, and SGLT2 inhibitor users on insulin. This allows clinically meaningful comparisons. The use of logistic regression and propensity score matching strengthens the analysis, although it cannot eliminate all confounding.
Limitations
The study is observational and cross-sectional. Therefore, it can show association but cannot establish causation. Exposure duration, dose-response relationships, drug switching, and exact temporal relationship between drug initiation and infection could not be fully standardised. Longitudinal glycaemic control and formal interaction analysis between glycaemic control and infection risk were not performed. UTI and GTI diagnoses were based on physician documentation in routine practice, but microbiological confirmation was not standardised across all centres.
These limitations are important. Patients receiving insulin or multiple-drug regimens may differ substantially from patients receiving SGLT2 inhibitor plus DPP4 inhibitor alone. Therefore, the lower infection incidence seen with the SGLT2i–DPP4i combination should be viewed as a hypothesis-generating observation requiring prospective validation, not as a final conclusion that DPP4 inhibitors prevent infections.
CME INDIA clinical pearls
- In this large Indian real-world study of 15,611 people with type 2 diabetes, the overall six-month incidence of UTI and/or genital tract infection was 11.3%.
- SGLT2 inhibitor users had significantly more urogenital infections than non-users: 13.2% versus 7.2%.
- The genital infection signal was stronger than the UTI signal: GTI was 7.5% in SGLT2 inhibitor users versus 2.3% in non-users.
- Women, elderly patients, obese individuals, patients with CKD, and those with longer diabetes duration require closer counselling and follow-up.
- The most interesting finding was the lower observed infection incidence when SGLT2 inhibitors were combined with DPP4 inhibitors, especially in the group using only SGLT2i plus DPP4i.
- This DPP4i signal is clinically intriguing but not causal proof. It should be tested prospectively.
- The study supports continued use of SGLT2 inhibitors with better patient selection, hygiene counselling, early symptom recognition, and structured follow-up.
Final CME INDIA takeaway
This Indian multicentre real-world study confirms a clinically important reality: SGLT2 inhibitors are associated with increased urogenital infection risk in type 2 diabetes, particularly genital tract infections. However, the research also provides an important new signal: the addition of DPP4 inhibitors to SGLT2 inhibitor therapy was associated with a lower observed incidence of UTI/GTI than SGLT2 inhibitor regimens without DPP4 inhibitors. The finding should not immediately change prescribing algorithms as a proven protective strategy, but it should influence how clinicians think about combination therapy, risk stratification, and future research.
The practical message for Indian diabetes care is clear: do not deny the cardiorenal benefits of SGLT2 inhibitors because of infection fear; instead, prescribe with precision, counsel with clarity, identify vulnerable patients early, and treat urogenital symptoms promptly. This study strengthens the case for Indian real-world evidence guiding Indian diabetes practice.
[All infographics created on Notebook LM, AI can make mistakes]
CME INDIA Tail-Piece
Reference:
Singh N.K., Singh A.K., Gupta A. et al. Real-world evidence of urinary tract infections and genital tract infections with sodium-glucose cotransporter-2 inhibitors alone or in combination with dipeptidyl peptidase-4 inhibitors in individuals with type-2 diabetes mellitus in India. BMC Endocrine Disorders, 2026. DOI: 10.1186/s12902-026-02304-z.
https://link.springer.com/article/10.1186/s12902-026-02304-z
Discover CME INDIA

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs