

CME INDIA Case Presentation by Dr. Karuturi Subrahmanyam, Consultant Physician, Kify Hospital, Rajahmundry, Andhra Pradesh, India.
CME INDIA Case Study
Abstract
Background: IgA Vasculitis (IgAV), formerly Henoch-Schönlein Purpura (HSP), is predominantly recognized as a pediatric condition. Adult-onset IgAV is rare, frequently relapsing, and carries a higher burden of gastrointestinal and renal morbidity. Gastrointestinal involvement without concurrent active purpura creates a profound diagnostic challenge, particularly in patients with comorbidities that confound the clinical picture.
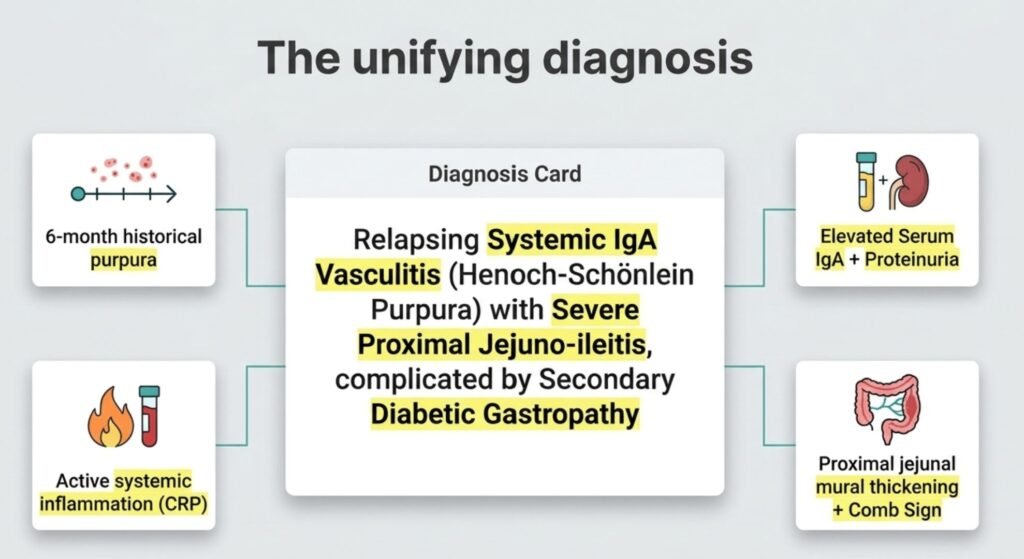
Case Presentation: A 46-year-old woman with Type 2 Diabetes Mellitus and Hypertension presented with six months of intractable vomiting and loose motions refractory to empirical treatment. A history of evanescent purpura and arthralgia six months prior, coinciding with symptom onset, was the critical historical anchor. Investigations revealed systemic inflammation (CRP 40.58 mg/L), mild leukocytosis, borderline elevated serum IgA (401 mg/dL), and proteinuria. Colonoscopy was unremarkable. MDCT Enterography demonstrated circumferential mural thickening (8.9 mm) over a 40–60 cm proximal jejunal segment with the radiologic “Comb Sign,” consistent with active mesenteric vasculitis. Serological exclusion of ANCA-associated vasculitis and SLE supported the diagnosis of relapsing systemic IgA Vasculitis with severe proximal jejuno-ileitis.
Management: Intravenous Methylprednisolone under a strict insulin infusion protocol produced clinical remission within 48 hours. The patient was transitioned to oral Prednisolone with Mycophenolate Mofetil as a steroid-sparing agent.
Conclusion: This case underscores that in adults, IgAV may present months after the initial cutaneous event, with gastrointestinal manifestations dominating the clinical picture. A normal colonoscopy does not exclude small bowel vasculitis. MDCT Enterography is the pivotal diagnostic tool when proximal small bowel disease is suspected.
Keywords: IgA vasculitis, Henoch-Schönlein Purpura, adult HSP, jejuno-ileitis, MDCT Enterography, Comb Sign, vasculitic enteritis, diabetic gastropathy.
1. Introduction
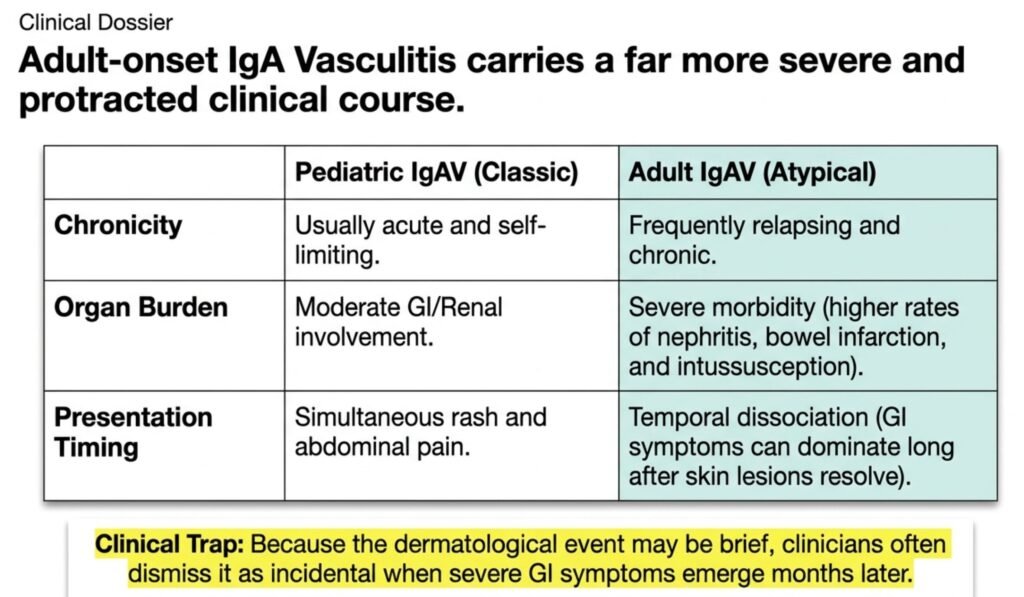
IgA Vasculitis (IgAV), formerly designated Henoch-Schönlein Purpura, is a small-vessel vasculitis characterized by IgA1-dominant immune deposits affecting the skin, joints, gastrointestinal tract, and kidneys. While it remains the most common systemic vasculitis in children, adult-onset IgAV accounts for a minority of cases and is associated with a significantly more severe and protracted course, with higher rates of renal impairment and gastrointestinal complications. [1,2]
Gastrointestinal involvement occurs in 50–75% of pediatric cases, typically manifesting as colicky abdominal pain, nausea, vomiting, and melena. In adults, GI manifestations may be the dominant or even the sole presentation at relapse, occurring long after the index cutaneous event has resolved. This temporal dissociation between purpura and GI symptoms represents one of the most treacherous diagnostic pitfalls in internal medicine. [3,4]
Comorbid conditions such as Type 2 Diabetes Mellitus further obscure the clinical landscape. Diabetic gastropathy and autonomic neuropathy can independently cause nausea, vomiting, and diarrhea, rendering the attribution of GI symptoms to an underlying vasculitic process particularly difficult. [5]
We present a case of relapsing IgA Vasculitis in a 46-year-old diabetic woman, in whom a six-month diagnostic odyssey was resolved by a detailed past history, targeted serology, and MDCT Enterography — and in whom a normal colonoscopy and a negative fecal calprotectin had initially provided false reassurance.
2. Case Presentation
2.1 History and Presenting Complaints
A 46-year-old woman, a known case of Type 2 Diabetes Mellitus (on oral hypoglycemic agents) and Hypertension (on antihypertensives), was admitted to Kify Hospital, Rajahmundry, with a six-month history of persistent vomiting and loose motions. Multiple courses of empirical antibiotics and anti-motility agents at peripheral centers had provided no sustained relief, and she had developed progressive constitutional weakness.
On detailed history, a pivotal finding emerged: approximately six months prior, coinciding with the onset of her gastrointestinal symptoms, she had experienced bilateral lower extremity erythematous spots (non-blanching, consistent with palpable purpura) and polyarthralgia. Both findings had resolved spontaneously and had not recurred at the time of presentation. This history had not been elicited at prior consultations.
2.2 Physical Examination
On admission, the patient was chronically ill-appearing but hemodynamically stable, with a blood pressure of 130/84 mmHg, heart rate of 88 bpm, and afebrile. Examination of the skin revealed no active purpura or rash. Abdominal examination demonstrated mid-abdominal tenderness on deep palpation, without guarding, rebound tenderness, or organomegaly. No peripheral lymphadenopathy was noted. Joint examination was unremarkable.
2.3 Laboratory Investigations
Key laboratory findings are summarized in Table 1.
| Parameter | Result | Reference Range |
| Hemoglobin | 10.4 g/dL | 12–16 g/dL |
| WBC Count | 11,700/μL | 4,000–11,000/μL |
| Platelet Count | Within normal limits | — |
| CRP | 40.58 mg/L | <5 mg/L |
| Serum IgA | 401 mg/dL | 70–400 mg/dL |
| PPBS | 245 mg/dL | <140 mg/dL |
| Urinalysis | Proteinuria 30 mg/dL | Negative |
| Fecal Calprotectin | 12.06 mg/kg | <50 mg/kg (negative) |
| ANA Profile (dsDNA, ENA) | Negative | Negative |
| p-ANCA (MPO) / c-ANCA (PR3) | Negative | Negative |
| Blood Culture | No growth | — |
| Stool (Ova & Parasites) | Negative | — |
| Clostridium difficile Toxin | Negative | — |
Table 1. Summary of laboratory investigations at admission.
Notably, serum IgA was borderline-elevated at 401 mg/dL (upper limit of normal 400 mg/dL), a finding that, when interpreted in conjunction with the clinical history, carried significant diagnostic weight.
2.4 Endoscopic Evaluation
Colonoscopy with intubation of the terminal ileum was performed. The entire colonic mucosa and terminal ileum appeared endoscopically normal, with no ulceration, erythema, or vascular abnormalities. Biopsies from representative sites showed no histological evidence of inflammatory bowel disease or vasculitis.
2.5 MDCT Enterography
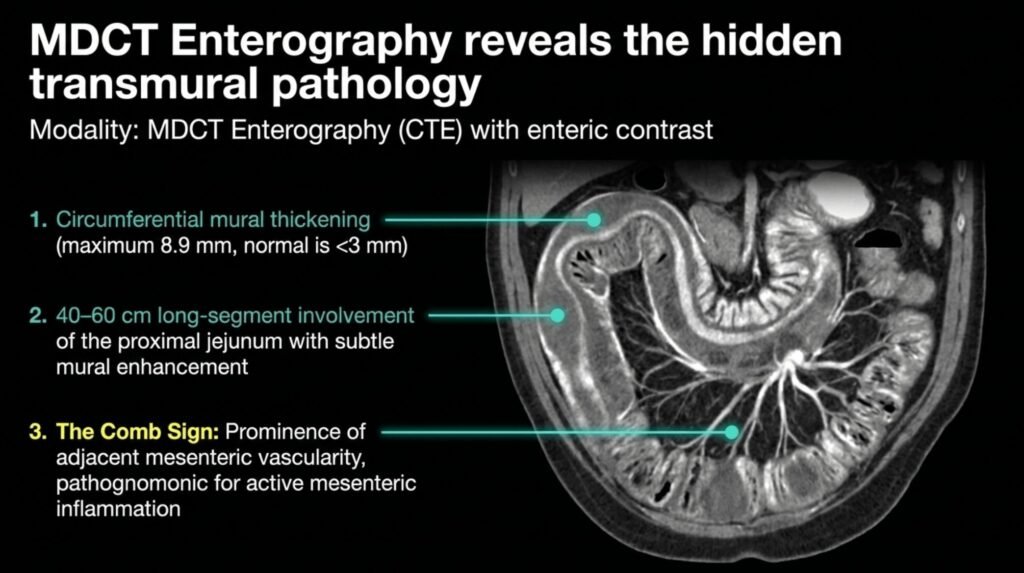
Given the proximal nature of symptoms (predominant vomiting) and the failure of colonoscopy to provide a diagnosis, MDCT Enterography (CTE) was performed with enteric contrast. This examination revealed:
- Circumferential mural thickening of a 40–60 cm segment of the proximal jejunum, with a maximum wall thickness of 8.9 mm (normal <3 mm).
- Subtle mural enhancement on post-contrast sequences, consistent with hyperemic bowel wall.
- Prominence of adjacent mesenteric vascularity, producing the radiologic “Comb Sign” — pathognomonic for active mesenteric inflammation.
- No mass lesion, lymphadenopathy with necrotic change, or distal obstruction identified.
The long-segment, circumferential, proximal jejunal involvement with the Comb Sign, in a patient with a history of purpura and an elevated IgA, was considered near-diagnostic of vasculitic enteritis.
3. Differential Diagnosis
The clinical constellation was considered against the following diagnostic possibilities:
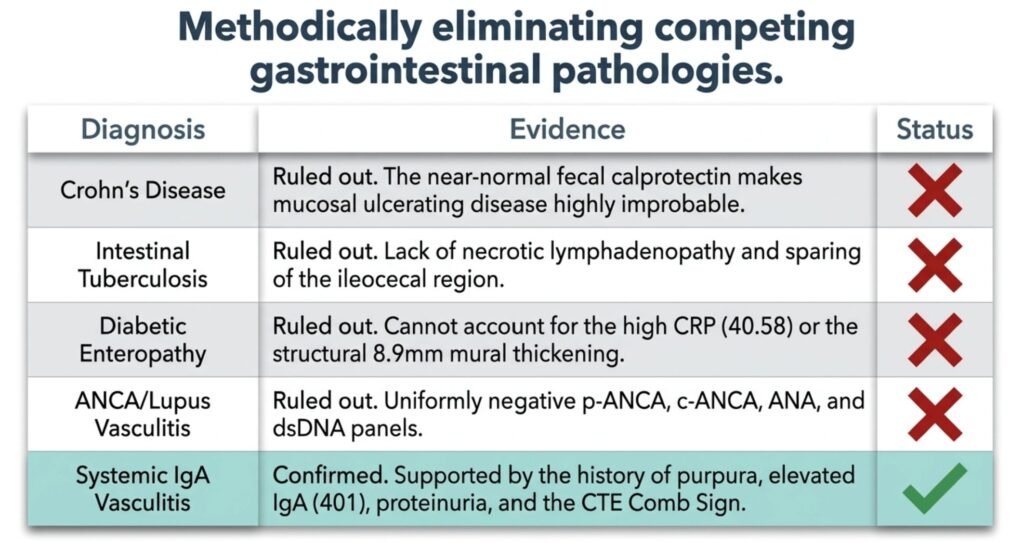
Crohn’s Disease (Jejuno-ileitis): Although standard colonoscopy was normal, “skip” proximal small bowel involvement is recognized in Crohn’s disease. However, Crohn’s classically produces mucosal ulceration, which elevates fecal calprotectin reliably; the near-normal calprotectin (12.06 mg/kg) rendered this less probable. [6]
Intestinal Tuberculosis: A relevant consideration in endemic regions. Intestinal TB typically involves the ileocecal region and is associated with necrotic mesenteric lymphadenopathy on imaging. Neither was present in this case. [7]
Diabetic Enteropathy: Long-standing hyperglycemia can produce dysmotility, diarrhea, and nausea. However, diabetic enteropathy is a diagnosis of exclusion and cannot account for a CRP of 40.58 mg/L or the structural circumferential mural thickening demonstrated on CTE. [5]
ANCA-Associated Vasculitis (GPA/MPA): Small-vessel vasculitis of the GPA/MPA spectrum can produce bowel wall thickening and systemic inflammation. This was excluded by a negative p-ANCA/MPO and c-ANCA/PR3 on ELISA. [8]
Systemic Lupus Erythematosus (Lupus Enteritis): SLE may cause mural edema and mesenteric vasculitis. The uniformly negative ANA profile, including dsDNA and ENA, effectively excluded this diagnosis. [9]
IgA Vasculitis (HSP) — Working Diagnosis: The convergence of (i) a six-month history of self-resolving palpable purpura, (ii) borderline-elevated serum IgA, (iii) proteinuria, (iv) active systemic inflammation, and (v) proximal jejunal mural thickening with the Comb Sign, in the absence of any alternative explanation, established IgAV as the unifying diagnosis. Adult IgAV is recognized to relapse with predominant gastrointestinal involvement in the absence of active skin disease. [2,3]
4. Final Diagnosis
Relapsing Systemic IgA Vasculitis (Henoch-Schönlein Purpura) with Severe Proximal Jejuno-ileitis, complicated by Secondary Diabetic Gastropathy.
5. Management and Outcome
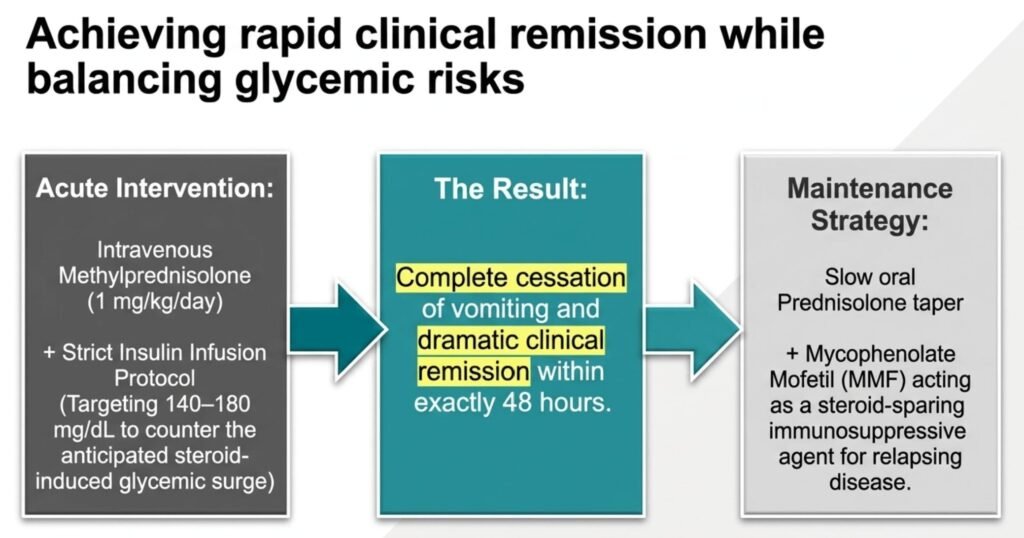
The patient was commenced on intravenous Methylprednisolone (1 mg/kg/day) under strict insulin infusion protocol, targeting blood glucose between 140–180 mg/dL to mitigate the anticipated steroid-induced glycemic surge.
Clinical response was rapid. Within 48 hours, vomiting ceased, oral intake improved, and serial CRP measurements demonstrated a downward trend toward normal.
Given her relapsing disease course, she was transitioned to a slow oral Prednisolone taper in combination with Mycophenolate Mofetil (MMF) as a steroid-sparing immunosuppressive agent, in accordance with the management approach for relapsing or steroid-dependent adult IgAV. [10]
Glycemic management was optimized with intensification of the insulin regimen given the dual challenge of steroid-induced hyperglycemia and baseline uncontrolled diabetes.
6. Discussion
6.1 Adult IgA Vasculitis: A More Severe Disease
Adult-onset IgAV differs fundamentally from its pediatric counterpart in disease severity, relapse frequency, and prognosis. Adults are more likely to develop nephritis, severe gastrointestinal complications including intussusception and bowel infarction, and a chronic relapsing course. [2] The dermatological event may be brief and self-limited, leading clinicians to dismiss it as incidental — as occurred during the initial consultations in this case.
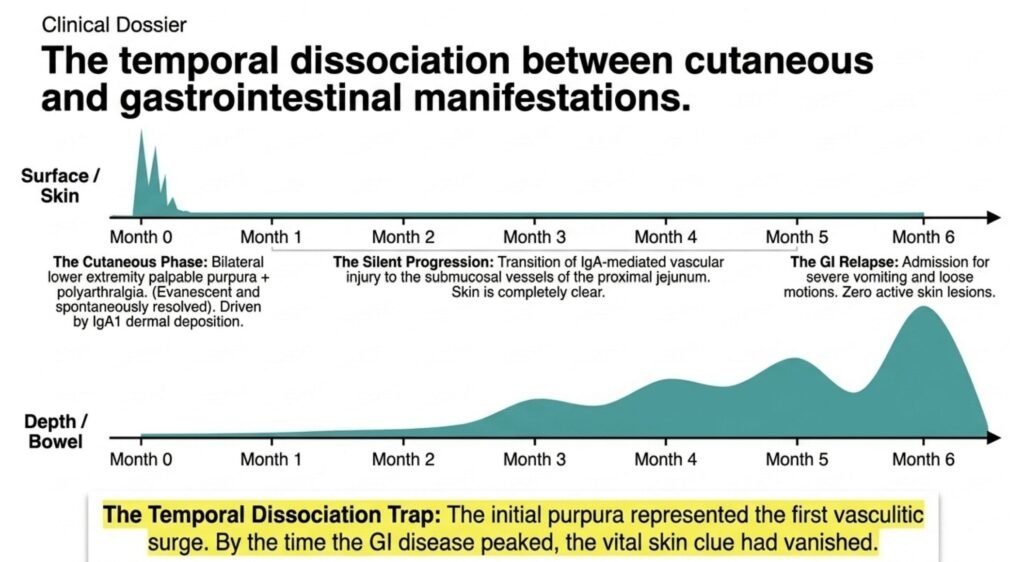
6.2 The “Skin-Bowel” Temporal Dissociation
A central teaching of this case is the prolonged interval between the cutaneous and gastrointestinal manifestations. The initial purpura represented the first vasculitic surge, driven by IgA1 immune complex deposition in dermal small vessels. With resolution of the cutaneous phase, ongoing IgA-mediated vascular injury in the submucosal vessels of the proximal jejunum perpetuated the gastrointestinal disease. This temporal dissociation has been documented in the literature and represents a major source of diagnostic delay in adult IgAV. [3,4]
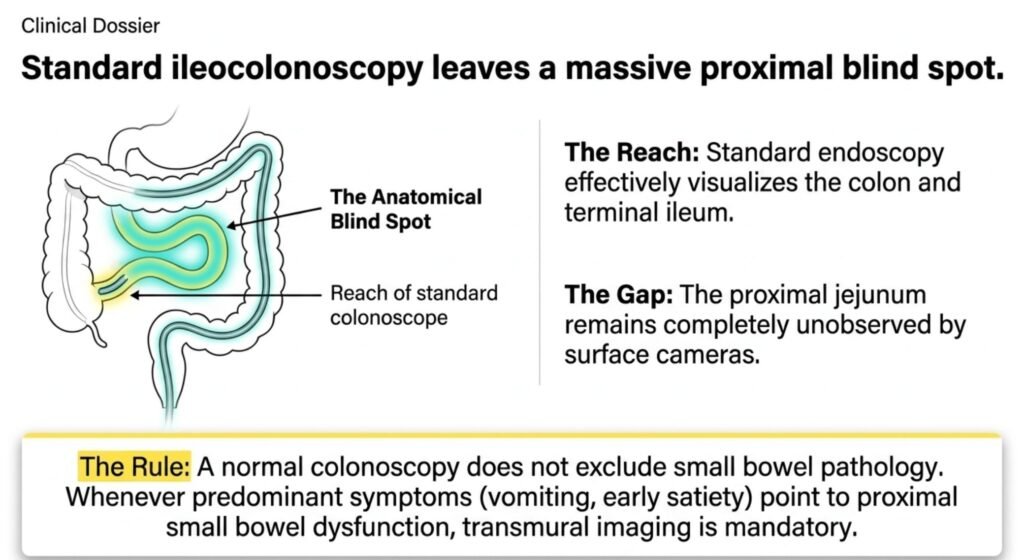
6.3 The Diagnostic Blind Spot of Colonoscopy
Standard ileocolonoscopy visualizes the colon and terminal ileum. The jejunum — particularly the proximal jejunum — lies beyond its reach. In this patient, a normal colonoscopy had been incorrectly interpreted as excluding significant small bowel pathology. Whenever the predominant symptoms point to proximal small bowel dysfunction (vomiting, early satiety, epigastric/mid-abdominal pain), MDCT Enterography is the mandatory imaging modality of choice, offering transmural and mesenteric detail inaccessible to standard endoscopy. [11]
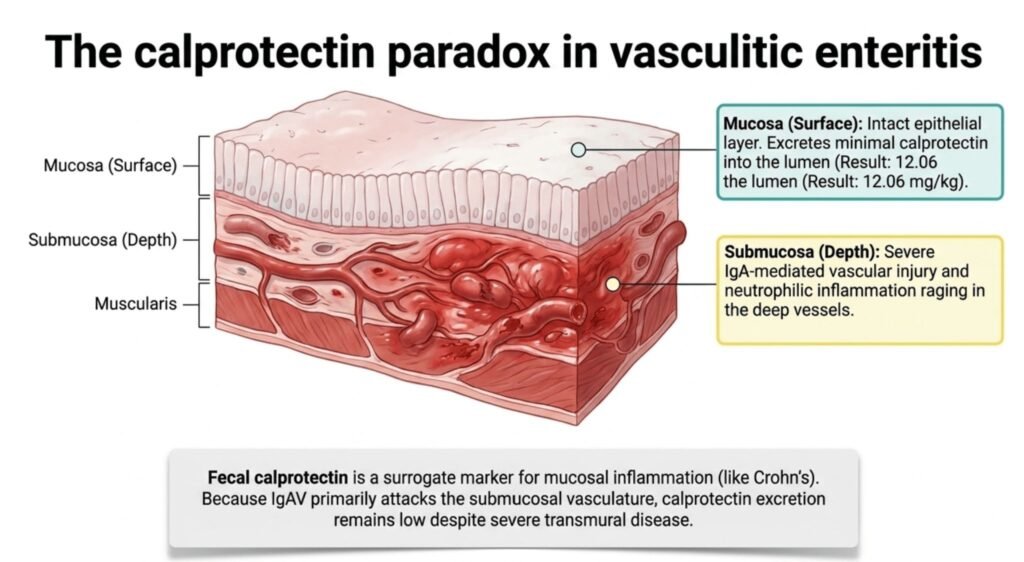
6.4 The Calprotectin Paradox
Fecal calprotectin is an established surrogate marker of mucosal neutrophilic inflammation, reliably elevated in inflammatory bowel disease. However, its utility in vasculitic enteritis is limited by a fundamental pathophysiological difference: in IgAV, the primary pathology is in the submucosal and muscularis vasculature, not the mucosa. When the epithelial layer remains intact, calprotectin excretion into the lumen remains low, producing a potentially false-negative result despite significant transmural disease. [12] Furthermore, jejunal calprotectin may be subject to enzymatic degradation during transit through the small and large bowel, further attenuating the signal. This “calprotectin paradox” must be recognized to avoid premature exclusion of transmural small bowel pathology.
6.5 Metabolic Comorbidity as a Disease Modifier
Chronic hyperglycemia contributes to a pro-inflammatory milieu and impairs vascular endothelial repair mechanisms, potentially amplifying the severity of vasculitic injury. In this patient, a postprandial blood glucose of 245 mg/dL reflected suboptimal glycemic control, which may have facilitated progression from an acute self-limiting vasculitic insult to a state of chronic mural edema and enteritis. Optimal glycemic control must be considered an integral component of the management of vasculitis in diabetic patients. [5]
6.6 A Note on Mycophenolate Mofetil
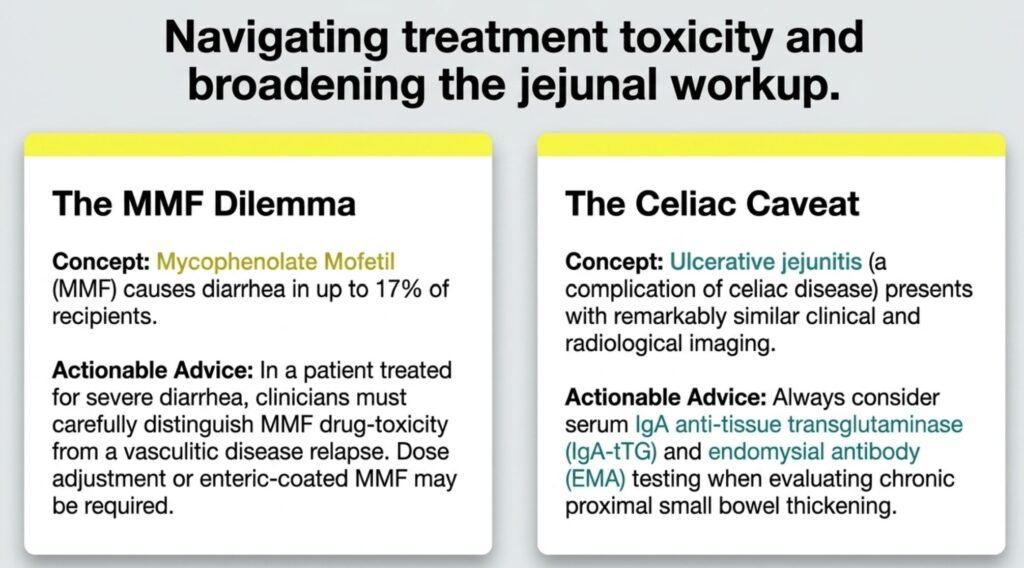
As correctly highlighted by Dr. Gunjan Joshi (Gastroenterology, Rajkot), Mycophenolate Mofetil carries a well-documented gastrointestinal adverse effect profile, with diarrhea occurring in up to 17% of recipients. [13] In a patient presenting with diarrhea as a primary complaint, the emergence or persistence of loose motions on MMF requires careful attribution — distinguishing drug-induced diarrhea from disease-related GI involvement. Close monitoring and, if necessary, dose adjustment or switching to enteric-coated MMF formulations is advisable. [13]
Additionally, as noted by Dr. Joshi, serum IgA anti-tissue transglutaminase (IgA-tTG) and endomysial antibody (EMA) testing should be considered in the evaluation of chronic jejunal pathology to exclude celiac disease and its complication of ulcerative jejunitis, which can present with a remarkably similar clinical and radiological picture. [14]
7. Learning Points
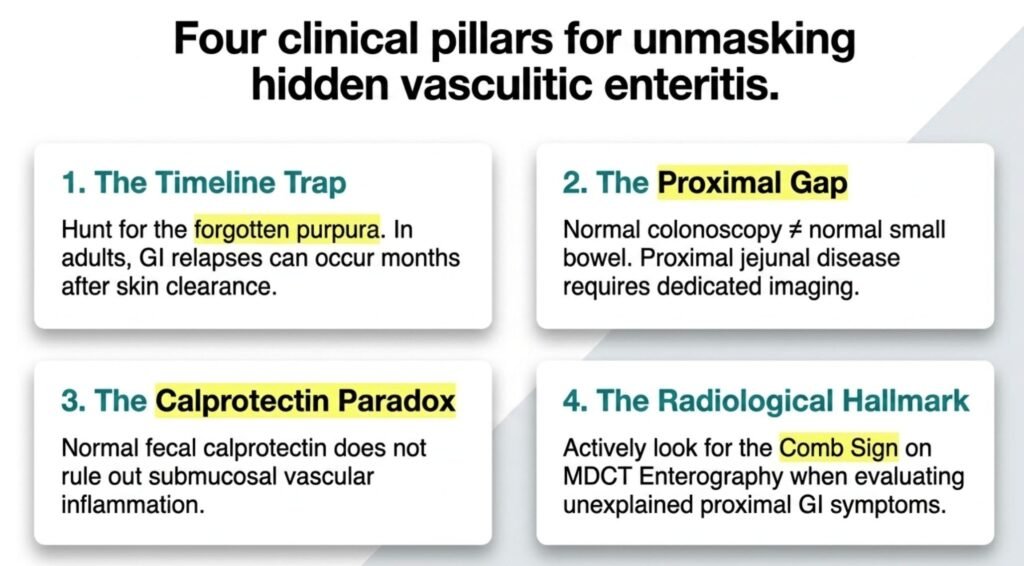
- The temporal dissociation trap: In adults, IgAV gastrointestinal relapse may occur months to years after the index cutaneous event, and often in the complete absence of active purpura. A meticulous past history remains the most powerful diagnostic instrument.
- Colonoscopy has a proximal limit: A normal ileocolonoscopy does not exclude small bowel disease. Proximal symptoms mandate small bowel imaging. MDCT Enterography is the investigation of choice.
- The calprotectin paradox: Fecal calprotectin measures mucosal, not transmural, inflammation. Vasculitis primarily involves submucosal vessels; a low calprotectin does not exclude significant small bowel vasculitic involvement.
- Diabetes as a disease amplifier: Uncontrolled hyperglycemia promotes a pro-inflammatory state and impairs resolution of vasculitic injury. Glycemic optimization is an essential component of therapy.
- The Comb Sign: Prominence of mesenteric vascularity (“Comb Sign”) on MDCT Enterography is a radiological hallmark of active mesenteric inflammation and, in the appropriate clinical context, should prompt consideration of vasculitic enteritis.
- Broaden the workup in jejunal disease: IgA-tTG and EMA should be included to exclude celiac disease and ulcerative jejunitis, especially when proximal small bowel thickening is identified.
8. Conclusion
This case exemplifies the diagnostic complexity of adult IgA Vasculitis presenting with dominant gastrointestinal manifestations in the quiescent phase of cutaneous disease. The key to diagnosis was not a sophisticated test but a careful clinical history — specifically, the recall of evanescent purpura six months prior. MDCT Enterography was the pivotal investigation that rendered the diagnosis visible. Clinicians must maintain a high index of suspicion for vasculitic enteritis when confronted with chronic proximal small bowel symptoms in a patient with any historical skin lesion, even one that has long resolved.
“Listen to the patient, look at the skin, and image the small bowel.”
References:
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1–11.
- Pillebout E, Thervet E, Hill G, Alberti C, Vanhille P, Nochy D. Henoch-Schönlein purpura in adults: outcome and prognostic factors. J Am Soc Nephrol. 2002;13(5):1271–1278.
- Saulsbury FT. Henoch-Schönlein purpura in children: report of 100 patients and review of the literature. Medicine (Baltimore). 1999;78(6):395–409.
- Uppal SS, Hussain MA, Al-Raqum HA, et al. Henoch-Schönlein’s purpura in adults versus children/adolescents: a comparative study. Clin Exp Rheumatol. 2006;24(2 Suppl 41):S26–30.
- Marathe CS, Rayner CK, Jones KL, Horowitz M. Relationships between gastric emptying, postprandial glycemia, and incretin hormones. Diabetes Care. 2013;36(5):1396–1405.
- Tibble JA, Sigthorsson G, Foster R, Forgacs I, Bjarnason I. Use of surrogate markers of inflammation and Rome criteria to distinguish organic from nonorganic intestinal disease. Gastroenterology. 2002;123(2):450–460.
- Debi U, Ravisankar V, Prasad KK, Sinha SK, Sharma AK. Abdominal tuberculosis of the gastrointestinal tract: revisited. World J Gastroenterol. 2014;20(40):14831–14840.
- Jennette JC, Falk RJ. Small-vessel vasculitis. N Engl J Med. 1997;337(21):1512–1523.
- Tian XP, Zhang X. Gastrointestinal involvement in systemic lupus erythematosus: insight into pathogenesis, diagnosis and treatment. World J Gastroenterol. 2010;16(24):2971–2977.
- Audemard-Verger A, Pillebout E, Guillevin L, Thervet E, Terrier B. IgA vasculitis (Henoch-Shönlein purpura) in adults: diagnostic and therapeutic aspects. Autoimmun Rev. 2015;14(7):579–585.
- Paulsen SR, Huprich JE, Fletcher JG, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. 2006;26(3):641–657.
- Tibble J, Bjarnason I. Fecal calprotectin as an index of intestinal inflammation. Drugs Today (Barc). 2001;37(2):85–96.
- Sollinger HW. Mycophenolate mofetil for the prevention of acute rejection in primary cadaveric renal allograft recipients. U.S. Renal Transplant Mycophenolate Mofetil Study Group. Transplantation. 1995;60(3):225–232.
- Rubio-Tapia A, Murray JA. Classification and management of refractory coeliac disease. Gut. 2010;59(4):547–557.
Correspondence: Dr. Karuturi Subrahmanyam, Consultant Physician, Kify Hospital, Rajahmundry, Andhra Pradesh, India.
Conflict of Interest: None declared.
Funding: None.
Patient Consent: Informed written consent was obtained from the patient for publication of this case report.
Acknowledgements: The authors thank Dr. Gunjan Joshi, Gastroenterologist, Rajkot, for his insightful peer commentary.
Discover CME INDIA:

- Explore CME INDIA Repository
- Examine CME INDIA Case Study
- Read History Today in Medicine
- Register for Future CMEs
Excellent work up of the case, meticulously arrived at a definitive diagnosis and managed well keei g in view the associated Type 2 Diabetes Mellitus. Kudos to all involved in the management of the case